

Randomized phase II study of the PDGFRα antibody olaratumab plus liposomal doxorubicin versus liposomal doxorubicin alone in patients with platinum-refractory or platinum-resistant advanced ovarian cancer
- PMID: 30591028
- PMCID: PMC6307114
- DOI: 10.1186/s12885-018-5198-4
Randomized phase II study of the PDGFRα antibody olaratumab plus liposomal doxorubicin versus liposomal doxorubicin alone in patients with platinum-refractory or platinum-resistant advanced ovarian cancer
Abstract
Background: Olaratumab is a platelet-derived growth factor receptor-α (PDGFRα)-targeting monoclonal antibody blocking PDGFRα signaling. PDGFRα expression is associated with a more aggressive phenotype and poor ovarian cancer outcomes. This randomized, open label phase II study evaluated olaratumab plus liposomal doxorubicin compared with liposomal doxorubicin alone in advanced ovarian cancer patients.
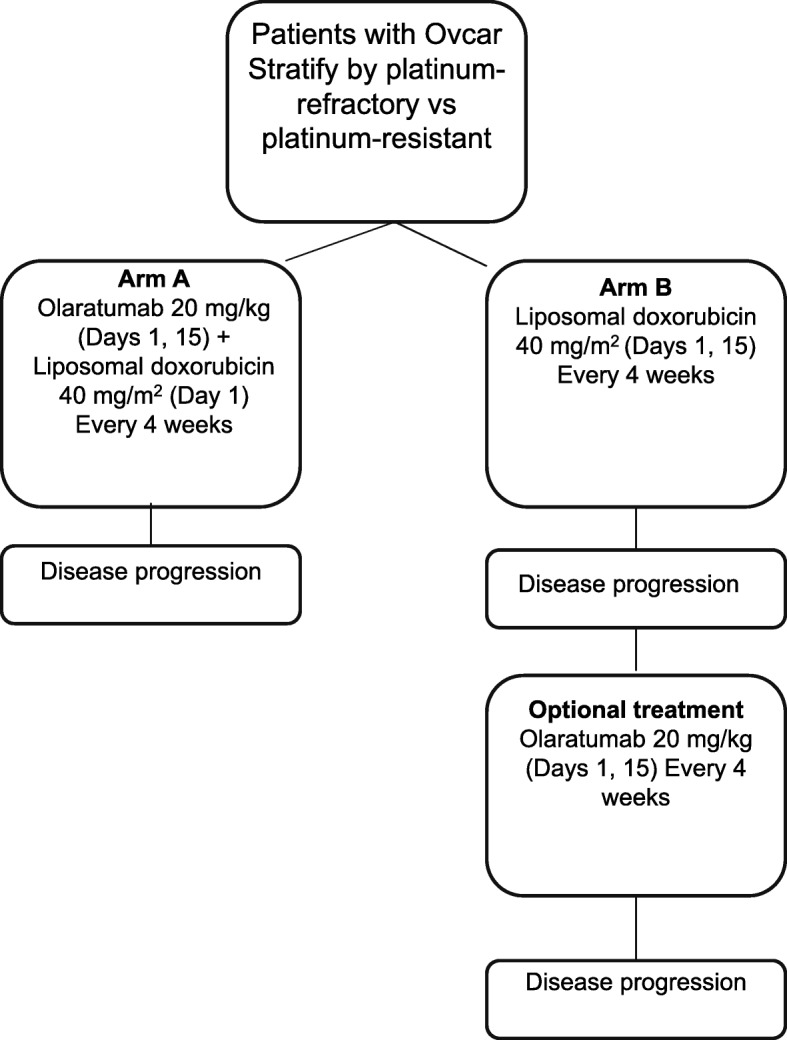
Methods: Patients with platinum-refractory or platinum-resistant advanced ovarian cancer were randomized 1:1 to receive liposomal doxorubicin (40 mg/m2, intravenous infusion) administered every 4 weeks with or without olaratumab (20 mg/kg, IV infusion) every 2 weeks. Patients were stratified based on prior response to platinum therapy (refractory vs resistant). The primary efficacy endpoint was progression-free survival (PFS). Secondary endpoints included overall survival (OS), objective response rate, duration of response, and safety.
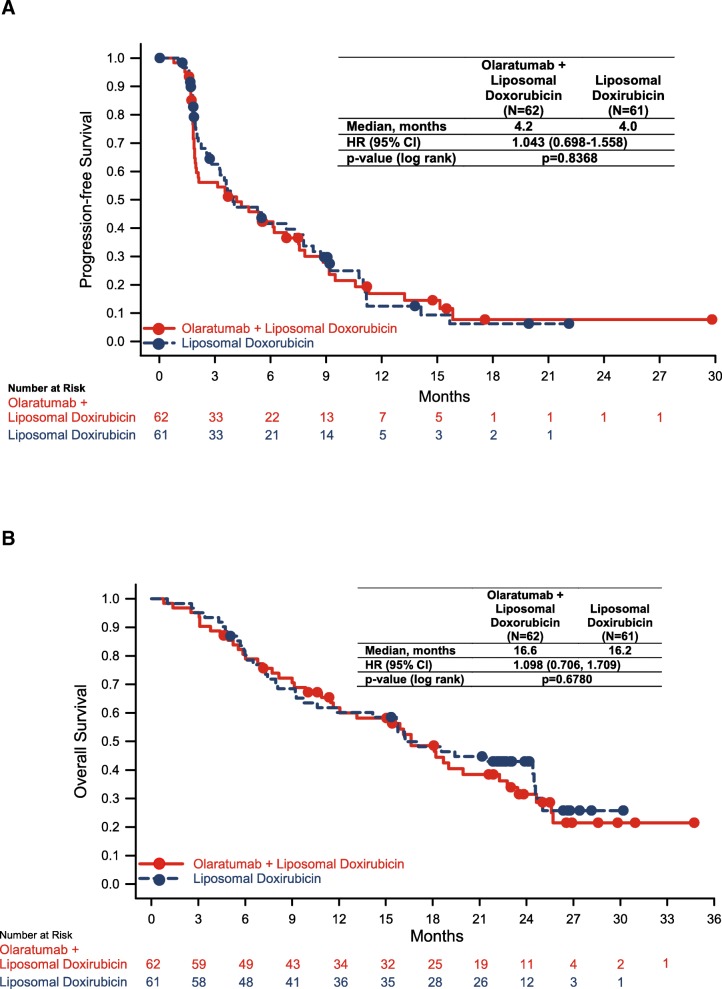
Results: A total of 123 patients were treated (62 olaratumab+liposomal doxorubicin; 61 liposomal doxorubicin). Median PFS was 4.2 months for olaratumab+liposomal doxorubicin and 4.0 months for liposomal doxorubicin (stratified hazard ratio [HR] = 1.043; 95% confidence interval [CI] 0.698-1.558; p = 0.837). Median OS was 16.6 months and 16.2 months in the olaratumab+liposomal doxorubicin and liposomal doxorubicin arms, respectively (HR = 1.098; 95% CI 0.71-1.71). In the platinum-refractory subgroup, median PFS was 5.5 months (95% CI 1.6-9.2) and 3.7 months (95% CI 1.9-9.2) in the olaratumab+liposomal doxorubicin (n = 15) and liposomal doxorubicin arms (n = 16), respectively (HR = 0.85; 95% CI 0.38-1.91). Overall, 59.7% (olaratumab+liposomal doxorubicin) and 65.6% (liposomal doxorubicin) of patients reported grade ≥ 3 adverse events regardless of causality. The most common treatment-emergent adverse events (all grades) regardless of causality were fatigue related (61%), nausea (57%), and constipation (52%) with olaratumab+liposomal doxorubicin and nausea (64%), fatigue related (62%), and mucositis (46%) with liposomal doxorubicin.
Conclusions: The addition of olaratumab to liposomal doxorubicin did not result in significant prolongation of PFS or OS in platinum-resistant or platinum-refractory ovarian cancer.
Trial registration: ClinicalTrials.gov identifier: NCT00913835 ; registered June 2, 2009.
Keywords: Liposomal doxorubicin; Olaratumab; Ovarian cancer; Platinum refractory; Platinum resistant.
Conflict of interest statement
Ethics approval and consent to participate
The study (NCT00913835) was conducted in accordance with the International Conference on Harmonisation Good Clinical Practice guidelines, the Declaration of Helsinki, and local laws and regulations. The study was approved by the following ethical review boards: Medstar Research Institute-Georgetown University Oncology Institutional Review Board; King’s Hospital Research Ethics Committee-King’s College Hospital; South East London Rec 3-King’s College Hospital; London–Dulwich Charing Cross Hospital; Henry Ford Health System.
Institutional Review Board; Indiana University-Purdue University Institutional Review Board; Dana Farber Cancer Institute Office for Human Research Studies; Dana Farber Cancer Institute Office for the Protection of Research Subjects; University of California–Irvine IRB; Chesapeake Research Review; Presbyterian Healthcare System Institutional Review Board; Hospital Clinico San Carlos, Servicio Farmacologia Clinica 1a planta Ala Norte–Ciudad Universitaria; Atlantic Health System, Institutional Review Board; University of Southern California IRB. All patients provided written informed consent.
Consent for publication
Not applicable.
Competing interests
WPM, MG, and ACH report no conflicts related to this manuscript. RTP reports research funding and SABs within de minimis.
PP, AS are employees of Eli Lilly and Company and own stock.
RI was an employee of Eli Lilly and Company at the time of manuscript preparation. He is currently employed by Celgene Corporation.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- American Cancer Society . Atlanta: American Cancer Society. 2018. Cancer Facts & Figures 2018.
-
- Treatment of invasive epithelial ovarian cancers, by stage. American Cancer Society, Atlanta. 2017. https://www.cancer.org/cancer/ovarian-cancer/treating/by-stage.html. Accessed 15 Jan 2018.
-
- NCCN Clinical Practice Guidelines in Oncology: Ovarian Cancer. Version 1.2018. National Comprehensive Cancer Network, Ft. Washington, PA. 2018. Accessed 20 Apr 2018.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
