

Speckle tracking imaging as a predictor of left ventricular remodeling 6 months after first anterior ST elevation myocardial infarction in patients managed by primary percutaneous coronary intervention
- PMID: 30591753
- PMCID: PMC6303382
- DOI: 10.1016/j.ehj.2018.06.006
Speckle tracking imaging as a predictor of left ventricular remodeling 6 months after first anterior ST elevation myocardial infarction in patients managed by primary percutaneous coronary intervention
Abstract
Acute myocardial infarction (AMI) remains a leading cause of morbidity and mortality worldwide. LV remodeling is an important factor in the pathophysiology of advancing heart failure (HF).
Aim of the work: To evaluate the value of speckle tracking imaging as a predictor of left ventricular remodeling 6 months after first anterior STEMI in patients managed by primary PCI.
Methodology: Eighty-five patients with first acute anterior STEMI underwent primary PCI. Patients were followed up for 6 months. Echocardiography was done within 48 h [1] Standard transthoracic 2D echocardiographic examination: LV internal dimensions and volumes, Left Ventricular EF, and Wall Motion Score Index: [2] LV peak systolic global longitudinal strain and Torsion dynamics were assessed. Echocardiography was repeated at 6 months LV volumes and EF were calculated. LV remodeling was defined as an increase in LV EDV ≥ 20% 6 months after infarction as compared to baseline data. Patients were then classified into Group I: did not develop LV remodeling. Group II: developed LV remodeling. Both groups were studied to determine predictors of LV remodeling.
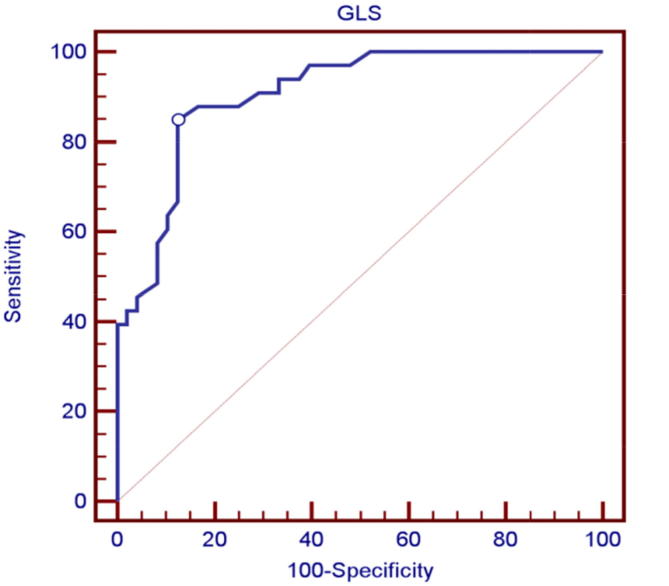
Results: At baseline echocardiographic evaluation there was no statistically significant difference between both groups regarding both LVEDD and LVEDV, while there was statistically significant increase in both LV ESD and LV ESV, with statistically significant lower Ejection Fraction, in LV remodeling group. There was also statistically significant higher LV peak systolic GLS values in LV remodeling group, the best cut-off value was >-12.5 (Sensitivity 87%, Specificity 85%) and LV torsion was also statistically significantly lower in the LV remodeling group, with the best cut-off value for LV torsion was <9.5°, [Sensitivity 91%, Specificity 85%].Independent predictors of LV remodeling after AMI: baseline WMSI > 1.8, baseline LV EF < 40, GLS > -12.5%, LV torsion < 9.5°, CK-MB > 500 U/L, baseline Thrombus grade > 4 and total ischemic time.
Conclusion: Average peak systolic GLS and LV torsion at echocardiography done early after myocardial infarction are independent predictors of LV remodeling after anterior STEMI and can be used to predict occurrence of LV remodeling after 6 months.
Keywords: Left ventricular remodeling; Remodeling; Speckle tracking.
Figures







Similar articles
-
Left ventricular torsion assessed by two-dimensional echocardiography speckle tracking as a predictor of left ventricular remodeling and short-term outcome following primary percutaneous coronary intervention for acute myocardial infarction: A single-center experience.Echocardiography. 2017 Aug;34(8):1159-1169. doi: 10.1111/echo.13611. Epub 2017 Jul 28. Echocardiography. 2017. PMID: 28752661
-
Value of three-dimensional strain parameters for predicting left ventricular remodeling after ST-elevation myocardial infarction.Int J Cardiovasc Imaging. 2017 May;33(5):663-673. doi: 10.1007/s10554-016-1053-3. Epub 2017 Feb 1. Int J Cardiovasc Imaging. 2017. PMID: 28150084
-
Reverse left ventricular remodeling after acute myocardial infarction: the prognostic impact of left ventricular global torsion.Int J Cardiovasc Imaging. 2013 Apr;29(4):787-95. doi: 10.1007/s10554-012-0159-5. Epub 2012 Nov 22. Int J Cardiovasc Imaging. 2013. PMID: 23179752
-
Reduced left ventricular torsion early after myocardial infarction is related to left ventricular remodeling.Circ Cardiovasc Imaging. 2010 Jul;3(4):433-42. doi: 10.1161/CIRCIMAGING.109.926196. Epub 2010 May 17. Circ Cardiovasc Imaging. 2010. PMID: 20478987
-
The value of echocardiography in the staging of preexcitation syndrome and the assessment of left ventricular wall dyskinesia in children.Front Pediatr. 2025 Apr 25;13:1567172. doi: 10.3389/fped.2025.1567172. eCollection 2025. Front Pediatr. 2025. PMID: 40352602 Free PMC article. Review.
Cited by
-
The Value of Three-Dimensional Speckle-Tracking Echocardiography in the Prediction of Cardiovascular Events in Patients with Hypertension Complicated by Acute Myocardial Infarction: A Long-Term Follow-Up Study.Int J Gen Med. 2021 Oct 12;14:6703-6712. doi: 10.2147/IJGM.S330789. eCollection 2021. Int J Gen Med. 2021. PMID: 34675631 Free PMC article.
References
-
- Bolooki H.M., Askar A. Disease management project. Cardiology, Acute Myocardial Infarction, Cleveland Clinic. 2010
-
- Konstam M.A., Kramer D.G., Patel A.R. Left ventricular remodeling in heart failure: Current concepts in clinical significance and assessment. JACC Cardiovasc Imaging. 2011;4:98–108. - PubMed
-
- Thygesen K., Alpert J.S., White H.D. The writing group on behalf of the joint ESC/ACCF/AHA/WHF task force for the universal definition of myocardial infarction. Eur Heart J. 2012;33:2551–2567. - PubMed
-
- James P.A., Oparil S., Carter B.L., Cushman W.C. Evidence-based guideline for the management of high blood pressure in adults report from the panel members appointed to the eighth joint national committee (JNC 8) JAMA. 2014;311:507–520. - PubMed
-
- Tominaga M. Diagnostic criteria for diabetes mellitus. RinshoByori. 1999;47(10):901–908. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous