

Insulin resistance influences the impact of hypertension on left ventricular diastolic dysfunction in a community sample
- PMID: 30592058
- PMCID: PMC6712340
- DOI: 10.1002/clc.23145
Insulin resistance influences the impact of hypertension on left ventricular diastolic dysfunction in a community sample
Abstract
Background: Although obesity-associated metabolic abnormalities (insulin resistance-IR) may not play as marked a role in determining left ventricular (LV) diastolic dysfunction (DD) as hypertension, the impact of combinations of these risk factors on DD is unknown.
Hypothesis: We hypothesized that IR influences the impact of hypertension on DD.
Methods: In 704 randomly selected participants from a community sample with a high prevalence of hypertension (50.6%) and obesity (46.5%), we determined adiposity indices, IR from the homeostasis model (HOMA-IR) and LV diastolic function using standard echocardiographic techniques.
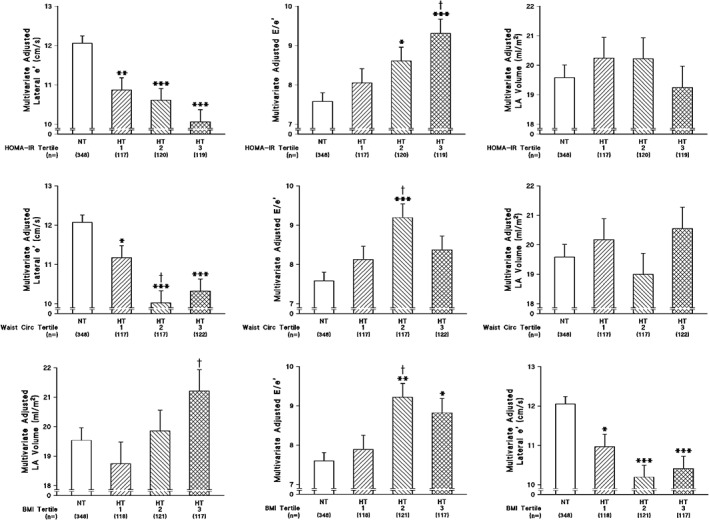
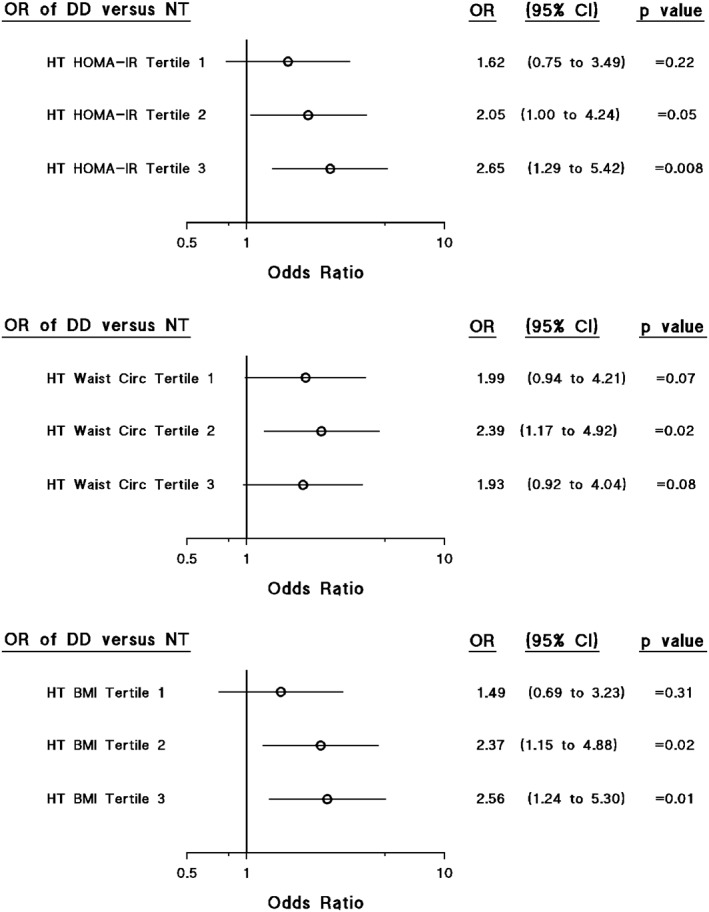
Results: HOMA-IR was independently associated with lateral wall e' and E/e' (P < 0.05 to P < 0.005) as well as a diagnosis of DD (P < 0.02). Importantly, however, an enhanced relationship between HOMA-IR and E/e' in hypertensives (n = 356, partial r = 0.15, P < 0.005) as compared to normotensives (n = 348, partial r = 0.02 P = 0.75) was noted. Consequently, as compared to normotensives, with adjustments for confounders, hypertension was independently associated with DD only in those with the highest tertile of HOMA-IR (odds ratio = 2.65, 95% confidence interval = 1.29-5.42, P < 0.01), while in those with the lowest tertile of HOMA-IR, hypertension failed to show a higher prevalence of DD (P = 0.22).
Conclusions: Insulin resistance enhances the impact of hypertension on LV DD. Thus, DD is more likely to occur with the combination of hypertension and IR.
Keywords: hypertension; insulin resistance; left ventricular diastolic function; obesity.
© 2018 The Authors. Clinical Cardiology Published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflict of interests.
Figures
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251‐259. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, et al. Outcomes of heart failure with preserved ejection fraction in a population‐based study. N Engl J Med. 2006;355:260‐269. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
