

Peroxisome Proliferator-Activated Receptor-γ Knockdown Impairs Bone Morphogenetic Protein-2-Induced Critical-Size Bone Defect Repair
- PMID: 30593824
- PMCID: PMC6412314
- DOI: 10.1016/j.ajpath.2018.11.019
Peroxisome Proliferator-Activated Receptor-γ Knockdown Impairs Bone Morphogenetic Protein-2-Induced Critical-Size Bone Defect Repair
Abstract
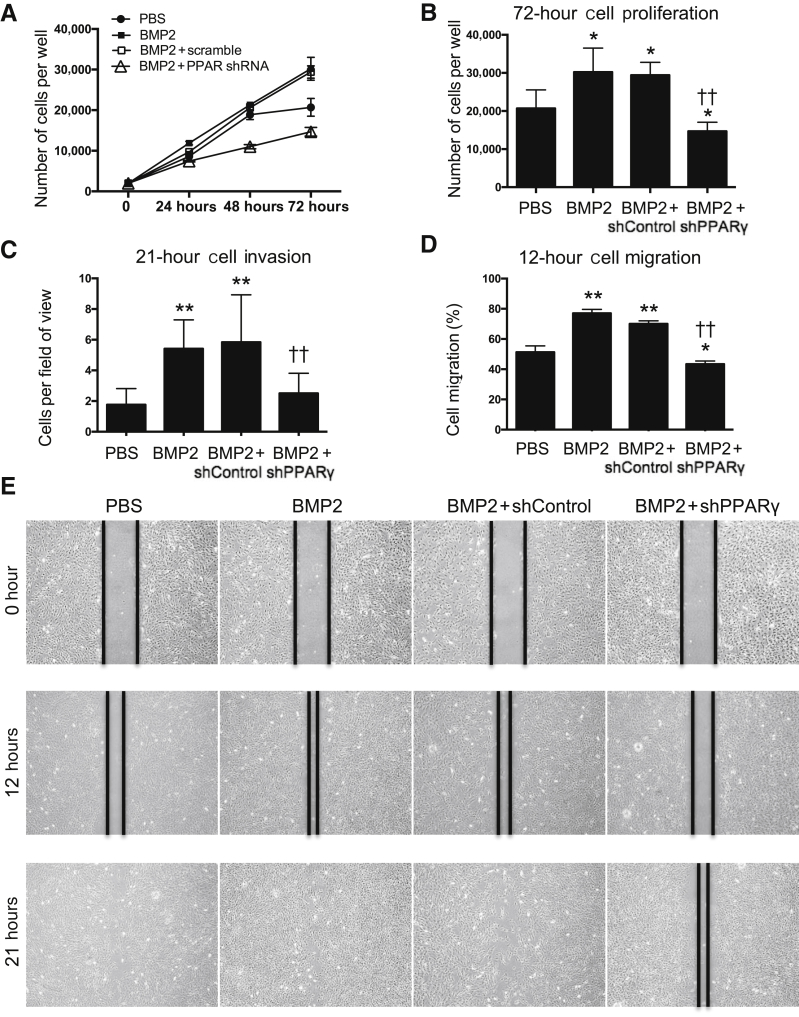
The Food and Drug Administration-approved clinical dose (1.5 mg/mL) of bone morphogenetic protein-2 (BMP2) has been reported to induce significant adverse effects, including cyst-like adipose-infiltrated abnormal bone formation. These undesirable complications occur because of increased adipogenesis, at the expense of osteogenesis, through BMP2-mediated increases in the master regulatory gene for adipogenesis, peroxisome proliferator-activated receptor-γ (PPARγ). Inhibiting PPARγ during osteogenesis has been suggested to drive the differentiation of bone marrow stromal/stem cells toward an osteogenic, rather than an adipogenic, lineage. We demonstrate that knocking down PPARγ while concurrently administering BMP2 can reduce adipogenesis, but we found that it also impairs BMP2-induced osteogenesis and leads to bone nonunion in a mouse femoral segmental defect model. In addition, in vitro studies using the mouse bone marrow stromal cell line M2-10B4 and mouse primary bone marrow stromal cells confirmed that PPARγ knockdown inhibits BMP2-induced adipogenesis; attenuates BMP2-induced cell proliferation, migration, invasion, and osteogenesis; and escalates BMP2-induced cell apoptosis. More important, BMP receptor 2 and 1B expression was also significantly inhibited by the combined BMP2 and PPARγ knockdown treatment. These findings indicate that PPARγ is critical for BMP2-mediated osteogenesis during bone repair. Thus, uncoupling BMP2-mediated osteogenesis and adipogenesis using PPARγ inhibition to combat BMP2's adverse effects may not be feasible.
Copyright © 2019 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures





References
-
- Giannoudis P.V., Dinopoulos H., Tsiridis E. Bone substitutes: an update. Injury. 2005;36 Suppl 3:S20–S27. - PubMed
-
- Yelin E.H., Trupin L.S., Sebesta D.S. Transitions in employment, morbidity, and disability among persons ages 51-61 with musculoskeletal and non-musculoskeletal conditions in the US, 1992-1994. Arthritis Rheum. 1999;42:769–779. - PubMed
-
- Alt V., Borgman B., Eicher A., Heiss C., Kanakaris N.K., Giannoudis P.V., Song F. Effects of recombinant human bone morphogenetic protein-2 (rhBMP-2) in grade III open tibia fractures treated with unreamed nails: a clinical and health-economic analysis. Injury. 2015;46:2267–2272. - PubMed
-
- Garrison K.R., Donell S., Ryder J., Shemilt I., Mugford M., Harvey I., Song F. Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review. Health Technol Assess. 2007;11:1–150. iii-iv. - PubMed
-
- Mendoza M.C., Sonn K.A., Kannan A.S., Bellary S.S., Mitchell S.M., Singh G., Park C., Yun C., Stock S.R., Hsu E.L., Hsu W.K. The effect of vancomycin powder on bone healing in a rat spinal rhBMP-2 model. J Neurosurg Spine. 2016;25:147–153. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
