

Risk and Temporal Changes of Heart Failure Among 5-Year Childhood Cancer Survivors: a DCOG-LATER Study
- PMID: 30595059
- PMCID: PMC6405698
- DOI: 10.1161/JAHA.118.009122
Risk and Temporal Changes of Heart Failure Among 5-Year Childhood Cancer Survivors: a DCOG-LATER Study
Abstract
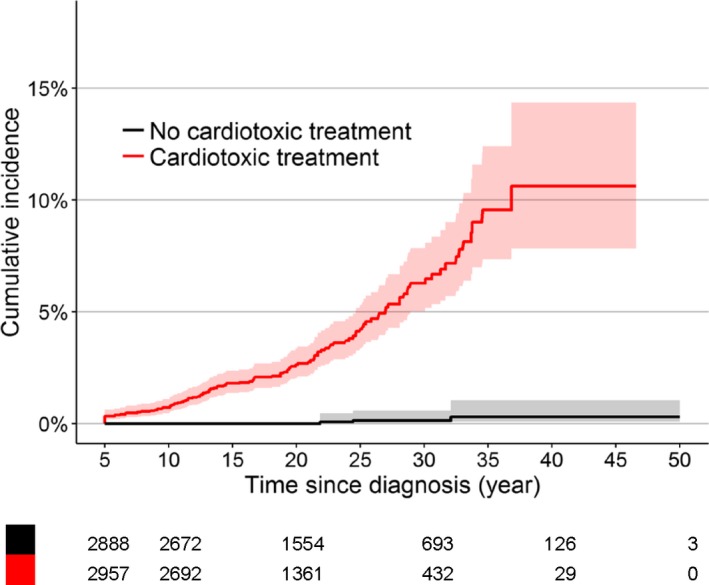
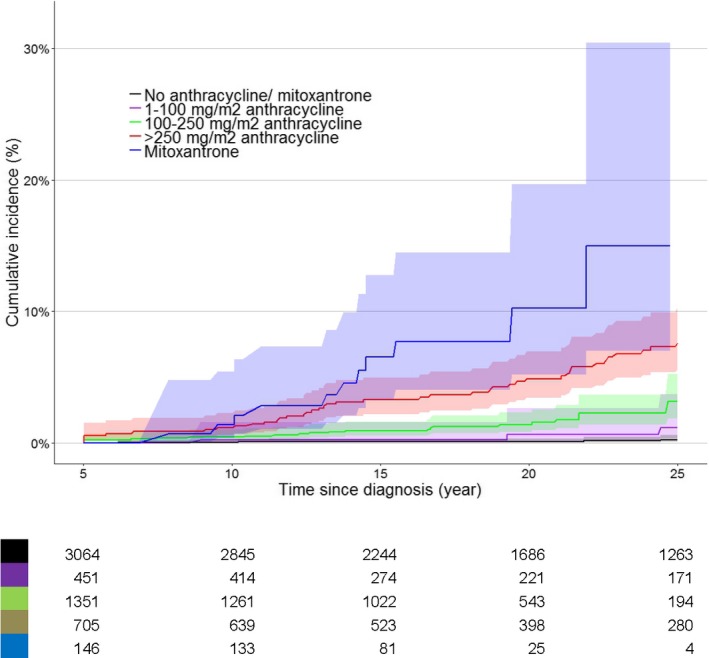
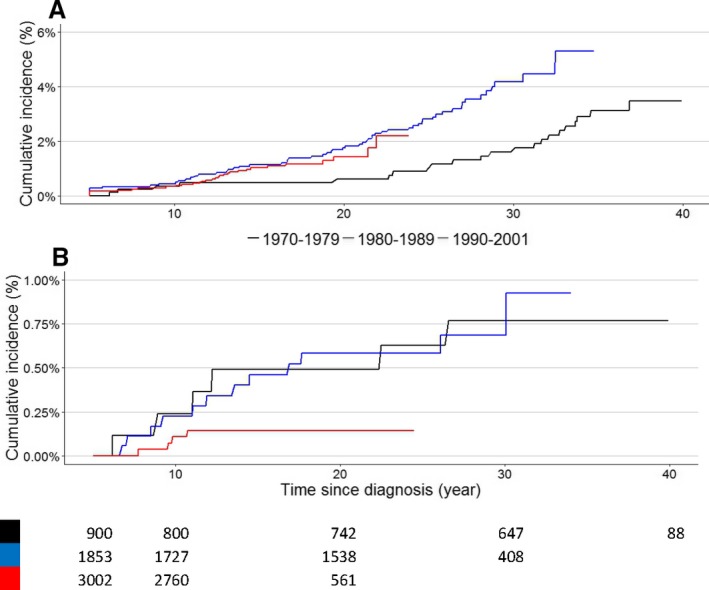
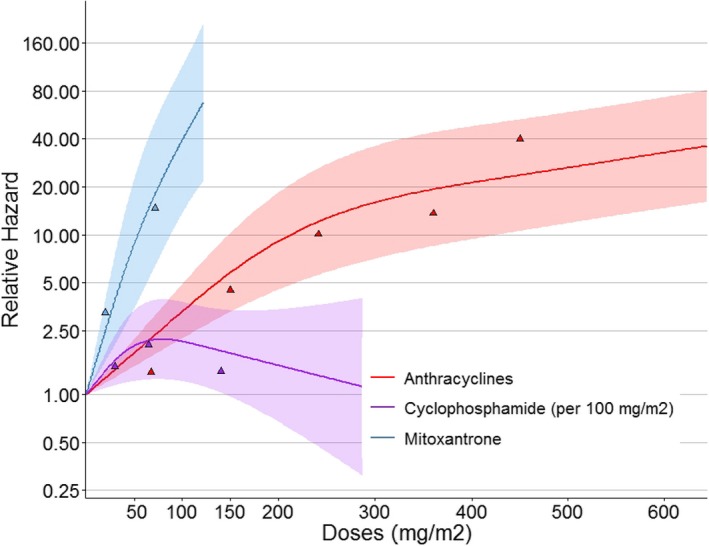
Background Heart failure is one of the most important late effects after treatment for cancer in childhood. The goals of this study were to evaluate the risk of heart failure, temporal changes by treatment periods, and the risk factors for heart failure in childhood cancer survivors ( CCS ). Methods and Results The DCOG-LATER (Dutch Childhood Oncology Group-Long-Term Effects After Childhood Cancer) cohort includes 6,165 5-year CCS diagnosed between 1963 and 2002. Details on prior cancer diagnosis and treatment were collected for this nationwide cohort. Cause-specific cumulative incidences and risk factors of heart failure were obtained. Cardiac follow-up was complete for 5,845 CCS (94.8%). After a median follow-up of 19.8 years and at a median attained age of 27.3 years, 116 survivors developed symptomatic heart failure. The cumulative incidence of developing heart failure 40 years after childhood cancer diagnosis was 4.4% (3.4%-5.5%) among all CCS. The cumulative incidence of heart failure grade ≥3 among survivors treated in the more recent treatment periods was higher compared with survivors treated earlier (Gray test, P=0.05). Mortality due to heart failure decreased in the more recent treatment periods (Gray test, P=0.02). In multivariable analysis, survivors treated with a higher dose of mitoxantrone or cyclophosphamide had a higher risk of heart failure than survivors who were exposed to lower doses. Conclusions CCS treated with mitoxantrone, cyclophosphamide, anthracyclines, or radiotherapy involving the heart are at a high risk for severe, life-threatening or fatal heart failure at a young age. Although mortality decreased, the incidence of severe or life-threatening heart failure increased with more recent treatment periods.
Keywords: childhood cancer survivors; heart failure.
Figures
References
-
- Curry HL, Parkes SE, Powell JE, Mann JR. Caring for survivors of childhood cancers: the size of the problem. Eur J Cancer. 2006;42:501–508. - PubMed
-
- Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, Friedman DL, Marina NM, Hobbie W, Kadan‐Lottick NS, Schwartz C, Leisenring W, Robison LL. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355:1572–1582. - PubMed
-
- Geenen MM, Cardous‐Ubbink MC, Kremer LC, van der Bos C, van der Pal HJ, Heinen RC, Jaspers MWM, Koning CC, Oldenburger F, Langeveld NE, Hart AAM, Bakker PJ, Caron HN, van Leeuwen FE. Medical assessment of adverse health outcomes in long‐term survivors of childhood cancer. JAMA. 2007;297:2705–2715. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
