

Transcatheter aortic valve replacement in India-Early experience, challenges, and outcomes from a single center
- PMID: 30595287
- PMCID: PMC6309715
- DOI: 10.1016/j.ihj.2018.09.012
Transcatheter aortic valve replacement in India-Early experience, challenges, and outcomes from a single center
Abstract
Background: Despite the increasing popularity of transcatheter aortic valve replacement (TAVR), only about 10,000 TAVR cases have been performed in Asia to date. The procedure is still in a nascent stage in India with very few centers offering this state-of-art technique. Here, we present the early results of TAVR experience at our center.
Methods: Forty-nine patients with severe symptomatic aortic stenosis (AS) were referred to our center for TAVR from November 2015 to February 2018. Twenty-five patients underwent TAVR at our conventional cardiac catheterization laboratory under local or general anesthesia, with standby surgical team support.
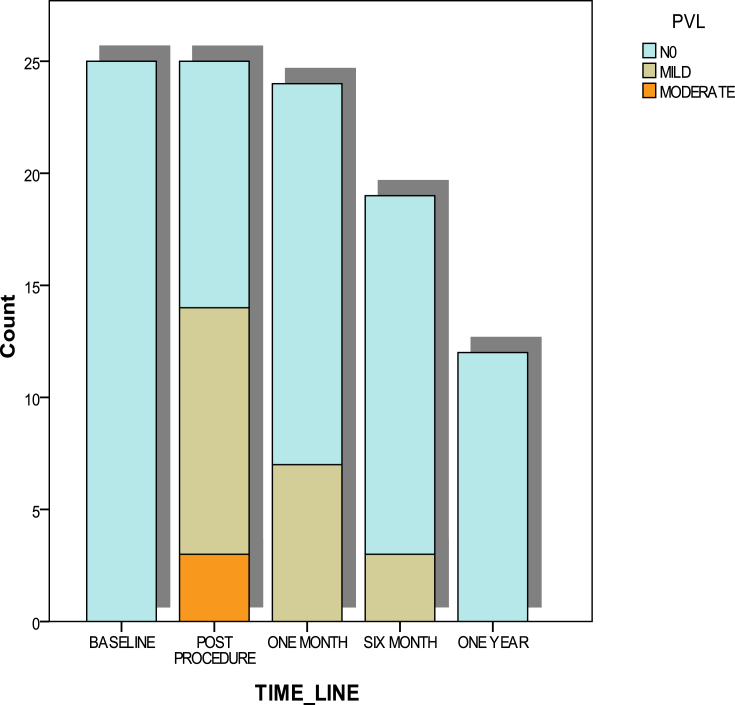
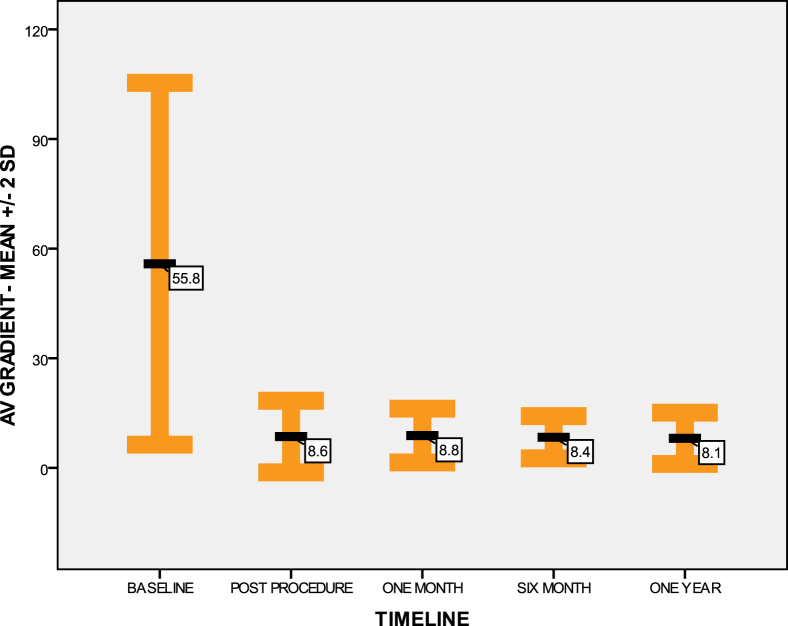
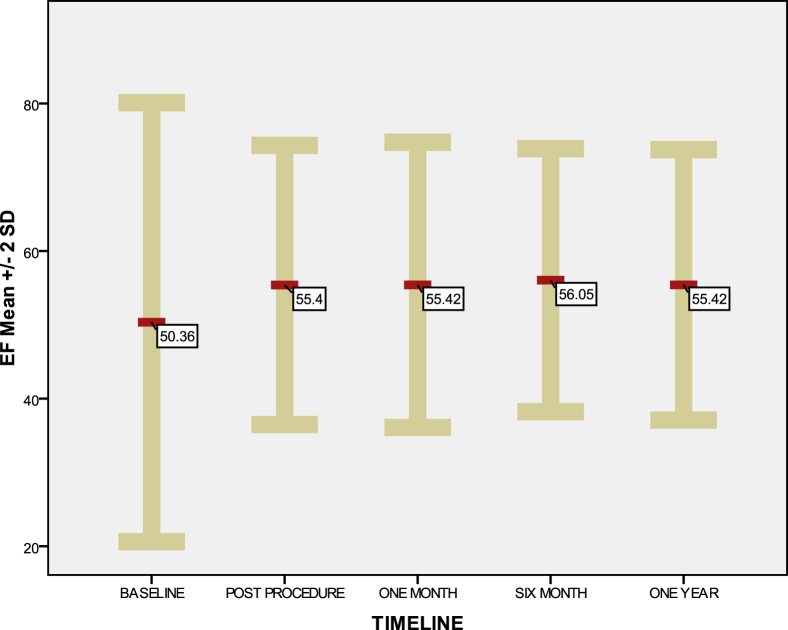
Results: The mean age of the patients was 72.0 ± 8.1 years. The mean Society of Thoracic Surgeons score was 13.8 ± 10.2. Baseline mean ejection fraction was 50.3 ± 14.8%. Baseline mean aortic valve gradient was 55.8 ± 24.7 mmHg. There was one procedural-related death. Two of the patients required urgent surgery: one for contained annular rupture and one underwent vascular repair for femoral artery occlusion. Mild and moderate paravalvular leak was seen in 11 and 3 patients, respectively. Four patients (16%) required permanent pacemaker. Eighty percent were in New York Heart Association class I-II at discharge. One-year all-cause mortality was 8%, with no hospitalizations or major adverse cardiac event during the 1-year follow-up.
Conclusion: Our early data clearly shows that in our country, TAVR is a good alternative for symptomatic severe AS for high surgical risk cases. Large-scale multicenter studies are required to study the real impact of TAVR in the Indian scenario. During initial years of implementation of a nationwide TAVR program, it may be prudent to focus on creating TAVR Centers of Excellence by developing an ideal hub and spokes model.
Keywords: Aortic stenosis; Indian experience; Transcatheter aortic valve replacement (TAVR).
Copyright © 2018 Cardiological Society of India. Published by Elsevier B.V. All rights reserved.
Figures

References
-
- Osnabrugge R.L.J., Mylotte D., Head S.J. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modelling study. J Am Coll Cardiol. 2013;62(11):1002–1012. - PubMed
-
- Vahanian A., Alfieri O., Andreotti F. Guidelines on the management of valvular heart disease (version 2012): the joint task force on the management of valvular heart disease of the European society of cardiology (ESC) and the European association for cardio-thoracic surgery (EACTS) Eur J Cardio Thorac Surg. 2012;42:S1–S44. - PubMed
-
- Leon M.B., Smith C.R., Mack M., Miller D.C., Moses J.W. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607. - PubMed
-
- Smith C.R., Leon Martin B., Mack Michael J., Craig Miller D., Moses Jeffrey W. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–2198. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
