

Simultaneous stoma reinforcement and perineal reconstruction with biological mesh - A multicentre prospective observational study
- PMID: 30595839
- PMCID: PMC6308243
- DOI: 10.1016/j.amsu.2018.12.006
Simultaneous stoma reinforcement and perineal reconstruction with biological mesh - A multicentre prospective observational study
Abstract
Introduction: The optimal method for perineal reconstruction after extralevator abdominoperineal excision (elAPE) for low rectal cancer remains controversial. This study aimed to assess whether simultaneous perineal reconstruction and parastomal reinforcement with Strattice™ Reconstructive Tissue Matrix after elAPE could prevent hernia formation.
Methods: In this prospective, multicentre, observational, non-comparative study of consecutive patients undergoing elAPE for low rectal cancer underwent simultaneous perineal reconstruction and colostomy site reinforcement with Strattice™ mesh. All patients underwent long course chemoradiotherapy prior to surgery and had excision of the coccyx. Patients were assessed for perineal wound healing at 7 day, 1, 3, 6 and 12 months, perineal and parastomal hernia defects on clinical and radiological assessment at 1 year following surgery.
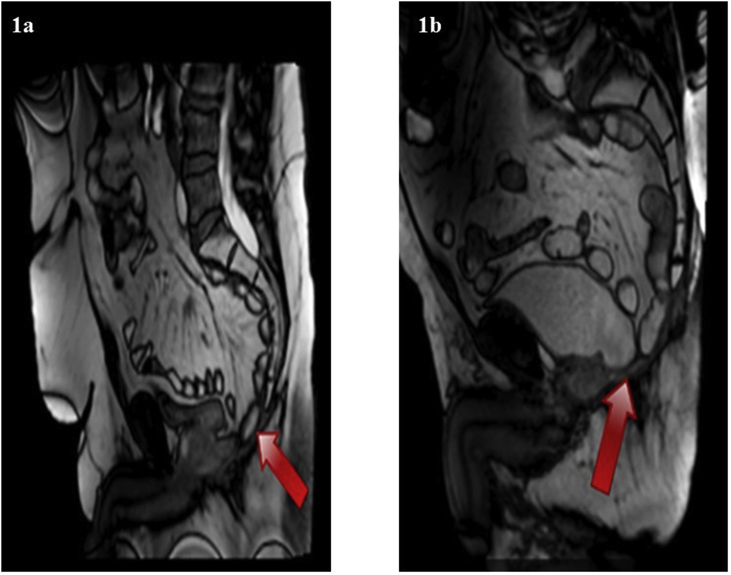
Results: 19 patients (median age = 67 years, median BMI = 26, M:F = 11:8) were entered the study. 10 (52.6%) patients underwent laparoscopic elAPE. The median length of post-operative stay was 9 days. Complete wound healing was observed for 8(42%) patients at 1 month, 12(63%) at 3 months, and 19(100%) patients at 12 months. Median time for radiological and clinical assessment for hernias was 12 months. No perineal hernia was detected in 17 patients following CT assessment. Dynamic MRI was undertaken in 11 patients at 12 months and all showed no evidence of perineal hernia. 3 (16%) patients had a parastomal hernia detected radiologically. No mesh was removed during the 12 months follow up period.
Conclusion: Perineal and parastomal reconstruction with biological mesh is a feasible approach for parastomal and perineal hernia prevention after laparoscopic and open elAPE.
Keywords: Abdominoperineal excision; Biological mesh; Dynamic MRI; Perineal hernia; Rectal cancer; Strattice; elAPE.
Figures
Similar articles
-
A low incidence of perineal hernia when using a biological mesh after extralevator abdominoperineal excision with or without pelvic exenteration or distal sacral resection in locally advanced rectal cancer patients.Tech Coloproctol. 2020 Aug;24(8):855-861. doi: 10.1007/s10151-020-02248-z. Epub 2020 Jun 8. Tech Coloproctol. 2020. PMID: 32514996 Free PMC article.
-
Biologic Mesh Reconstruction of the Pelvic Floor after Extralevator Abdominoperineal Excision: A Systematic Review.Front Surg. 2016 Feb 16;3:9. doi: 10.3389/fsurg.2016.00009. eCollection 2016. Front Surg. 2016. PMID: 26909352 Free PMC article. Review.
-
[Biological mesh versus primary closure for pelvic floor reconstruction following extralevator abdominoperineal excision: a meta-analysis].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Oct 25;24(10):910-918. doi: 10.3760/cma.j.cn.441530-20200509-00268. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 34674467 Chinese.
-
Biological mesh reconstruction versus primary closure for preventing perineal morbidity after extralevator abdominoperineal excision: a multicentre retrospective study.Colorectal Dis. 2020 Nov;22(11):1714-1723. doi: 10.1111/codi.15225. Epub 2020 Jul 26. Colorectal Dis. 2020. PMID: 32619064
-
Meta-analysis of biological mesh reconstruction versus primary perineal closure after abdominoperineal excision of rectal cancer.Int J Colorectal Dis. 2021 Mar;36(3):477-492. doi: 10.1007/s00384-020-03827-0. Epub 2021 Jan 3. Int J Colorectal Dis. 2021. PMID: 33392663 Review.
Cited by
-
Donor Site Morbidity of Patients Receiving Vertical Rectus Abdominis Myocutaneous Flap for Perineal, Vaginal or Inguinal Reconstruction.World J Surg. 2021 Jan;45(1):132-140. doi: 10.1007/s00268-020-05788-5. Epub 2020 Sep 29. World J Surg. 2021. PMID: 32995931 Free PMC article.
-
Comparison of different modalities for the diagnosis of parastomal hernia: a systematic review.Int J Colorectal Dis. 2020 Feb;35(2):199-212. doi: 10.1007/s00384-019-03499-5. Epub 2020 Jan 7. Int J Colorectal Dis. 2020. PMID: 31912267
-
Long-term outcomes of biological mesh repair following extra levator abdominoperineal excision of the rectum: an observational study of 100 patients.Tech Coloproctol. 2019 Aug;23(8):761-767. doi: 10.1007/s10151-019-02056-0. Epub 2019 Aug 7. Tech Coloproctol. 2019. PMID: 31392530 Free PMC article.
References
-
- Miles W.E. A method of performing abdomino-perineal excision for carcinoma of the rectum and of the terminal portion of the pelvic colon (1908) Ca - Cancer J. Clin. 1971;21(6):361. - PubMed
-
- Holm T. Extended abdominoperineal resection with gluteus maximus flap reconstruction of the pelvic floor for rectal cancer. Br. J. Surg. 2007;94(2):232–238. - PubMed
-
- Holm T. Controversies in abdominoperineal excision. Surg. Oncol. Clin. 2014;23(1):93–111. - PubMed
-
- Quirke P. Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision. Lancet. 1986;2(8514):996–999. - PubMed
LinkOut - more resources
Full Text Sources
