

Percutaneous fixation of thoracolumbar vertebral fractures
- PMID: 30595846
- PMCID: PMC6275852
- DOI: 10.1302/2058-5241.3.170026
Percutaneous fixation of thoracolumbar vertebral fractures
Abstract
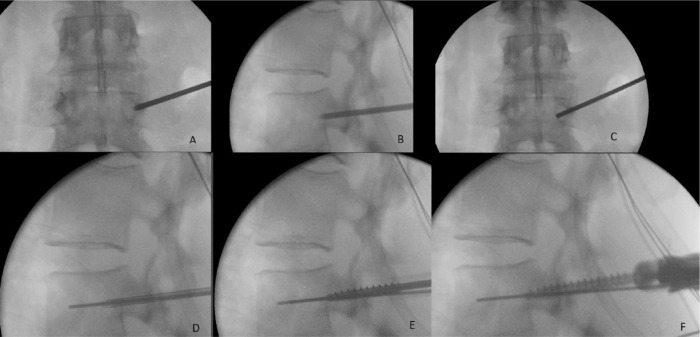
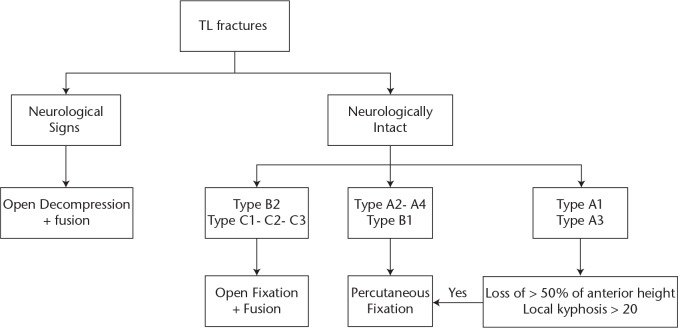
Surgical treatment of patients with thoracolumbar vertebral fracture without neurological deficit is still controversial.Management of vertebral fracture with percutaneous fixation was first reported in 2004.Advantages of percutaneous fixation are: less tissue dissection; decreased post-operative pain; decreased bleeding and operative time (depending on the steep learning curve); better screw positioning with fluoroscopy compared with an open freehand technique; and a decreased infection rate.The limitations of percutaneous fixation of vertebral fractures include increased radiation exposure to the patient and the surgeon, together with the steep learning curve for this technique.Adding a screw at the level of the fractured vertebra has the advantages of incorporating fewer motion segments with less operative time and bleeding. This also increases the axial, sagittal and torsional stiffness of the construct.Percutaneous fixation alone without grafting is sufficient for treating type A and B1 (AO classification) thoracolumbar fractures with satisfactory results concerning kyphosis reduction when compared with open instrumentation and fusion and with open fixation.Type C and B2 fractures (ligamentous injuries) should undergo fusion since the ligamentous healing is mechanically weak, increasing the risk of instability.This review offers a detailed description of percutaneous screw insertion and discusses the advantages and disadvantages. Cite this article: EFORT Open Rev 2018;3:604-613. DOI: 10.1302/2058-5241.3.170026.
Keywords: fracture stability; percutaneous fixation; thoracolumbar fractures.
Conflict of interest statement
ICMJE Conflict of interest statement: G. Riouallon declares payment for speaking and/or teaching and travel costs from Medtronic, activity outside the submitted work.
Figures




Similar articles
-
Percutaneous pedicle screw fixation through the pedicle of fractured vertebra in the treatment of type A thoracolumbar fractures using Sextant system: an analysis of 38 cases.Chin J Traumatol. 2010 Jun 1;13(3):137-45. Chin J Traumatol. 2010. PMID: 20515590
-
Treatment of unstable thoracolumbar junction fractures: short-segment pedicle fixation with inclusion of the fracture level versus long-segment instrumentation.Acta Neurochir (Wien). 2016 Oct;158(10):1883-9. doi: 10.1007/s00701-016-2907-0. Epub 2016 Aug 19. Acta Neurochir (Wien). 2016. PMID: 27541493
-
Comparison of clinical results between novel percutaneous pedicle screw and traditional open pedicle screw fixation for thoracolumbar fractures without neurological deficit.Int Orthop. 2019 Jul;43(7):1749-1754. doi: 10.1007/s00264-018-4012-x. Epub 2018 Jun 16. Int Orthop. 2019. PMID: 29909584 Clinical Trial.
-
Percutaneous fixation of thoracolumbar fractures: current concepts.Orthop Traumatol Surg Res. 2012 Dec;98(8):900-9. doi: 10.1016/j.otsr.2012.09.014. Epub 2012 Nov 17. Orthop Traumatol Surg Res. 2012. PMID: 23165222 Review.
-
Minimally invasive surgery for thoracolumbar spinal trauma.Ann Transl Med. 2018 Mar;6(6):102. doi: 10.21037/atm.2018.02.10. Ann Transl Med. 2018. PMID: 29707551 Free PMC article. Review.
Cited by
-
Outcome Measures of Open versus Minimally Invasive Surgery for Thoracolumbar Spinal Traumatic Fractures: A Systematic Review and Meta-Analysis.J Clin Med. 2024 Sep 19;13(18):5558. doi: 10.3390/jcm13185558. J Clin Med. 2024. PMID: 39337043 Free PMC article. Review.
-
Risk Factors for Postoperative Loss of Correction in Thoracolumbar Injuries Caused by High-Energy Trauma Treated via Percutaneous Posterior Stabilization without Bone Fusion.Medicina (Kaunas). 2022 Apr 24;58(5):583. doi: 10.3390/medicina58050583. Medicina (Kaunas). 2022. PMID: 35630000 Free PMC article.
-
Surgical management of thoracolumbar junction fractures: An evidence-based algorithm.World Neurosurg X. 2023 Jan 20;17:100151. doi: 10.1016/j.wnsx.2022.100151. eCollection 2023 Jan. World Neurosurg X. 2023. PMID: 36793355 Free PMC article.
-
Posterior Ligamentous Complex Injuries of the Thoracolumbar Spine: Importance and Surgical Implications.Cureus. 2021 Oct 14;13(10):e18774. doi: 10.7759/cureus.18774. eCollection 2021 Oct. Cureus. 2021. PMID: 34796064 Free PMC article. Review.
-
The Radiological Complications of Short-Segment Pedicle Screw Fixation Combined with Transforaminal Interbody Fusion in the Treatment of Unstable Thoracolumbar Burst Fracture: A Retrospective Case Series Study in Vietnam.Orthop Res Rev. 2022 Mar 29;14:91-99. doi: 10.2147/ORR.S356296. eCollection 2022. Orthop Res Rev. 2022. PMID: 35378735 Free PMC article.
References
-
- Melton LJ, Kallmes DF. Epidemiology of vertebral fractures: implications for vertebral augmentation. Acad Radiol 2006;13:538-545. - PubMed
-
- Wang H, Zhou Y, Li C, Liu J, Xiang L. Comparison of open versus percutaneous pedicle screw fixation using the sextant system in the treatment of traumatic thoracolumbar fractures. Clin Spine Surg 2017;30:E239-E246. - PubMed
-
- Irwin ZN, Arthur M, Mullins RJ, Hart RA. Variations in injury patterns, treatment, and outcome for spinal fracture and paralysis in adult versus geriatric patients. Spine 2004;29:796-802. - PubMed
LinkOut - more resources
Full Text Sources
