

Diagnosis and Treatment Algorithms of Acute Variceal Bleeding
- PMID: 30595875
- PMCID: PMC6284844
- DOI: 10.12865/CHSJ.43.03.02
Diagnosis and Treatment Algorithms of Acute Variceal Bleeding
Abstract
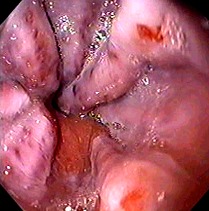
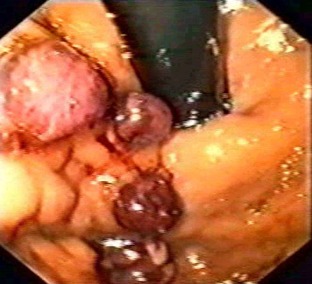
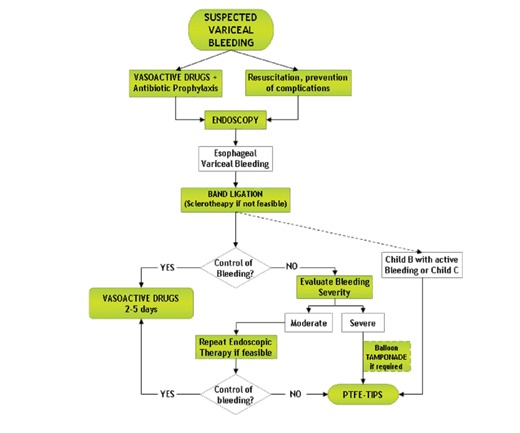
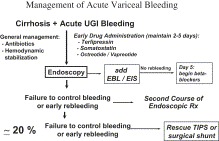
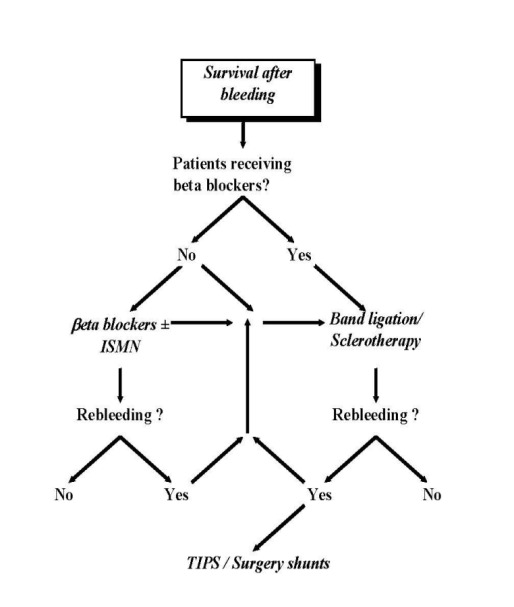
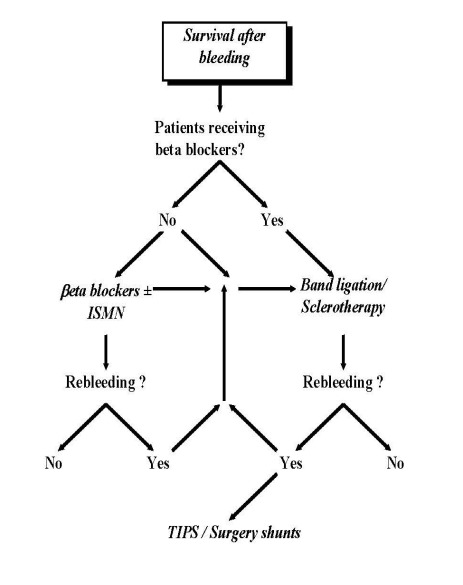
Esophageal varices are about 10%-15% of UGIB. Over 90% of patients with cirrhosis develop portal hypertension (PHT), but not all patients with PHT and liver cirrhosis have esophageal varices. At the time of diagnosis, only 60% of patients with cirrhosis have esophageal varices. In the case of variceal bleeding suspects, vasoactive drugs should be given as soon as possible and before endoscopy. Balloon tamponade is used to obtain temporary hemostasis by direct compression of hemorrhagic varices. The variceal band ligation is already the first place in the treatment and prevention of variceal bleeding, but also in rebleeding prevention. TIPS is used as a rescue therapy after failure of drug and endoscopic therapy. The mortality assigned to the hemorrhagic episode is substantially, estimated at 13-19% of the overall mortality in hepatic cirrhosis. Current recommendations for the treatment of acute variceal bleeding are the use of combination therapy: vasoactive drugs, balloon tamponade, elastic ligation and TIPS, whose staging is done in various diagnosis and treatment algorithms.
Keywords: endoscopy; portal hypertension; variceal bleeding.
Figures
References
-
- Jutabha R, Jensen DM. Management of upper gastrointestinal bleeding in the patient with chronic liver disease. Medical Clinics of North America. 1996;80(5):1035–1068. - PubMed
-
- Saftoiu A, Ciurea E. Hemoragiile digestive superioare non-variceale în gastroenterologie și hepatologie. București: Ed Medicală ; 2003. pp. 664–673.
-
- Garcia-Pagan JC, Bosch J. Medical treatment of portal hypertension. Bailliere Gastroenterol. 2000;14(6):895–909. - PubMed
-
- D'Amico G, Garcia-Tsao G, Cales P, Escorsell A, Nevens F, Cestari R. Diagnosis of portal hypertension: how and when . In: Franchis R, editor. Portal Hypertension. 3. Oxford, UK: Blackwell Science; 2001. pp. 36–64.
-
- D'Amico G, Pagliaro L, Bosch J. The treatment of portal hypertension: A meta-analytic review. Hepatology. 1995;22(1):332–354. - PubMed
Publication types
LinkOut - more resources
Full Text Sources