

Vancomycin Removal During High-Volume Peritoneal Dialysis in Acute Kidney Injury Patients: A Prospective Cohort Clinical Study
- PMID: 30596174
- PMCID: PMC6308823
- DOI: 10.1016/j.ekir.2018.09.014
Vancomycin Removal During High-Volume Peritoneal Dialysis in Acute Kidney Injury Patients: A Prospective Cohort Clinical Study
Abstract
Introduction: Vancomycin pharmacokinetic data in patients with acute kidney injury (AKI) on high-volume peritoneal dialysis (HVPD) are lacking. The aims were to study the pharmacokinetics of i.v. vancomycin in patients with AKI treated by HVPD who received an i.v. dose of vancomycin (15-20 mg/kg), to determine the vancomycin removal, and to establish vancomycin dosing and evaluation pharmacokinetics target attainment achievement for the empirical treatment of patients with AKI treated by HVPD.
Methods: Vancomycin was administered 1 hour before dialysis start. Samples of all dialysate were collected for a 24-hour period. Blood samples were collected after 1, 2, 4, and 24 hours of therapy. Vancomycin concentrations were determined using a liquid chromatographic (high-performance liquid chromatography)-fluorescence method. Pharmacokinetic calculations were completed assuming a 1-compartment model.
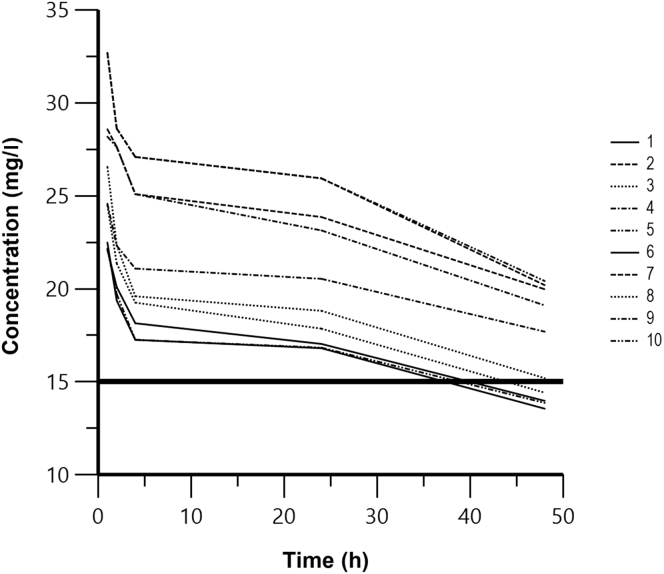
Results: Ten patients completed the study. The mean vancomycin dose administered was 18.0 ± 2.95 mg/kg (14.7-21.8 mg/kg) on the day of study (first day) and the mean percentage of vancomycin removal by HVPD was 21.7% ± 2.2% (16%-29%). Peritoneal clearance was 8.1 ± 2.2 ml/min (5.3-12 ml/min). The serum vancomycin half-life was 71.2 ± 24.7 hours (42-110 hours) during HVPD session, the maximum serum concentration was 26.2 ± 3.5 mg/l, which occurred 1 hour after vancomycin administration and HVPD start. Area under the curve (AUC)0-24/minimum inhibitory concentration (MIC) ratio ≥400 was achieved in all patients when MIC = 1 mg/l was considered.
Conclusion: HVPD removes considerable amounts of vancomycin in septic patients with AKI. Administration of 18 mg/kg vancomycin each 48 to 72 hours in patients with AKI undergoing HVPD was required to reach and maintain therapeutic concentrations.
Keywords: acute kidney injury; peritoneal dialysis; sepsis; vancomycin.
Figures
References
-
- Zarjou A., Agarwal A. Sepsis and acute kidney injury. J Am Soc Nephrol. 2011;22:999–1006. - PubMed
-
- Davenport A. Dialytic treatment for septic patients with acute kidney injury. Kidney Blood Press Res. 2011;34:218–224. - PubMed
-
- Uchino S., Bellomo R., Morimatsu H. Continuous renal replacement therapy: a worldwide practice survey. The beginning and ending supportive therapy for the kidney (B.E.S.T. kidney) investigators. Intensive Care Med. 2007;33:1563–1570. - PubMed
-
- Ostermann M., Joannidis M., Pani A. Patient selection and timing of continuous renal replacement therapy. Blood Purif. 2016;42:224–237. - PubMed
-
- Pannu N., Klarenbach S., Wiebe N. Renal replacement therapy in patients with acute renal failure: a systematic review. JAMA. 2008;299:793–805. - PubMed
