

Improving Care of STEMI in the United States 2008 to 2012
- PMID: 30596310
- PMCID: PMC6405711
- DOI: 10.1161/JAHA.118.008096
Improving Care of STEMI in the United States 2008 to 2012
Abstract
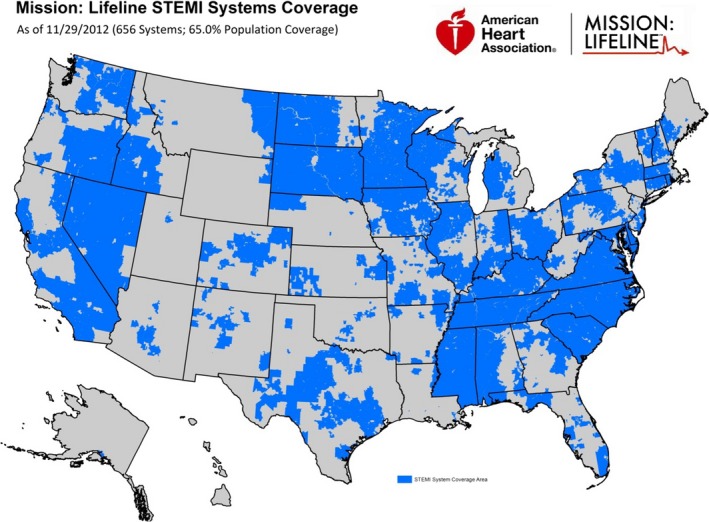
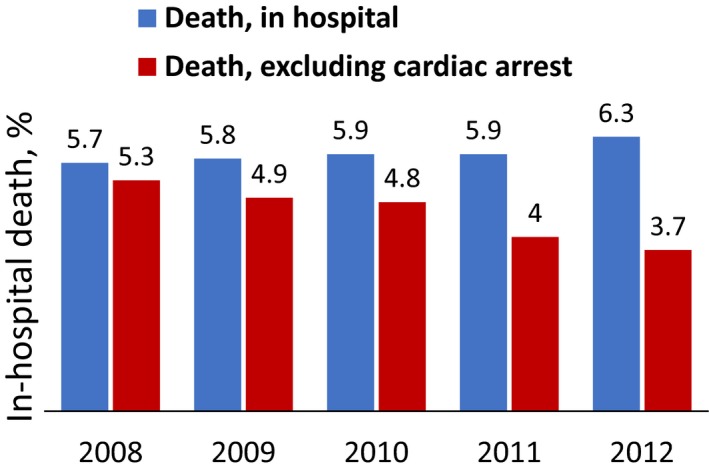
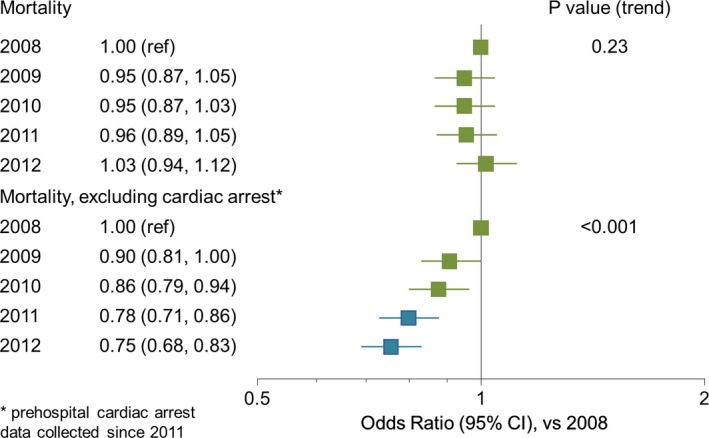
Background We aimed to determine the change in treatment strategies and times to treatment over the first 5 years of the Mission: Lifeline program. Methods and Results We assessed pre- and in-hospital care and outcomes from 2008 to 2012 for patients with ST -segment-elevation myocardial infarction at US hospitals, using data from the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network Registry-Get With The Guidelines Registry. In-hospital adjusted mortality was calculated including and excluding cardiac arrest as a reason for primary percutaneous coronary intervention delay. A total of 147 466 patients from 485 hospitals were analyzed. There was a decrease in the proportion of eligible patients not treated with reperfusion (6.2% versus 3.3%) and treated with fibrinolytic therapy (13.4% versus 7.0%). Median time from symptom onset to first medical contact was unchanged (≈50 minutes). Use of prehospital ECGs increased (45% versus 71%). All major reperfusion times improved: median first medical contact-to-device for emergency medical systems transport to percutaneous coronary intervention-capable hospitals (93 to 84 minutes), first door-to-device for transfers for primary percutaneous coronary intervention (130 to 112 minutes), and door-in-door-out at non-percutaneous coronary intervention-capable hospitals (76 to 62 minutes) (all P<0.001 over 5 years). Rates of cardiogenic shock and cardiac arrest, and overall in-hospital mortality increased (5.7% to 6.3%). Adjusted mortality excluding patients with known cardiac arrest decreased by 14% at 3 years and 25% at 5 years ( P<0.001). Conclusions Quality of care for patients with ST -segment-elevation myocardial infarction improved over time in Mission: Lifeline, including increased use of reperfusion therapy and faster times-to-treatment. In-hospital mortality improved for patients without cardiac arrest but did not appear to improve overall as the number of these high-risk patients increased.
Keywords: ST‐segment elevation myocardial infarction; fibrinolytic therapy; primary percutaneous coronary intervention; reperfusion.
Figures
Comment in
-
Excluding the Elephant in the Room: Cardiac Arrest.J Am Heart Assoc. 2019 Jan 8;8(1):e011381. doi: 10.1161/JAHA.118.011381. J Am Heart Assoc. 2019. PMID: 30595066 Free PMC article. No abstract available.
References
-
- Fibrinolytic Therapy Trialists’ (FTT) Collaborative Group . Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Lancet. 1994;343:311–322. - PubMed
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. - PubMed
-
- Jacobs AK, Antman EM, Faxon DP, Gregory T, Solis P. Development of systems of care for ST‐elevation myocardial infarction patients: executive summary. Circulation. 2007;116:217–230. - PubMed
-
- Jollis JG, Granger CB, Henry TD, Antman EM, Berger PB, Moyer PH, Pratt FD, Rokos IC, Acuña AR, Roettig ML, Jacobs AK. Systems of care for ST‐segment‐elevation myocardial infarction: a report from the American Heart Association's Mission: Lifeline. Circ Cardiovasc Qual Outcomes. 2012;5:423–428. - PubMed
-
- American Heart Association . Mission: Lifeline website. Available at: http://www.heart.org/HEARTORG/HealthcareResearch/MissionLifelineHomePage.... Accessed April 4, 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
