

Validation of the Clinical Index of Stable Febrile Neutropenia (CISNE) model in febrile neutropenia patients visiting the emergency department. Can it guide emergency physicians to a reasonable decision on outpatient vs. inpatient treatment?
- PMID: 30596803
- PMCID: PMC6312365
- DOI: 10.1371/journal.pone.0210019
Validation of the Clinical Index of Stable Febrile Neutropenia (CISNE) model in febrile neutropenia patients visiting the emergency department. Can it guide emergency physicians to a reasonable decision on outpatient vs. inpatient treatment?
Abstract
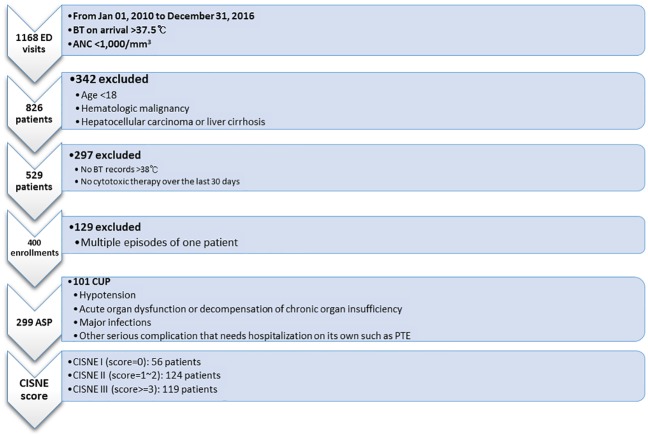
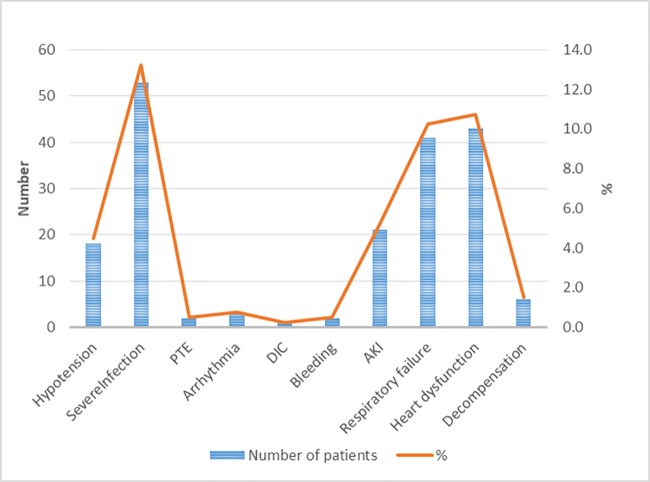
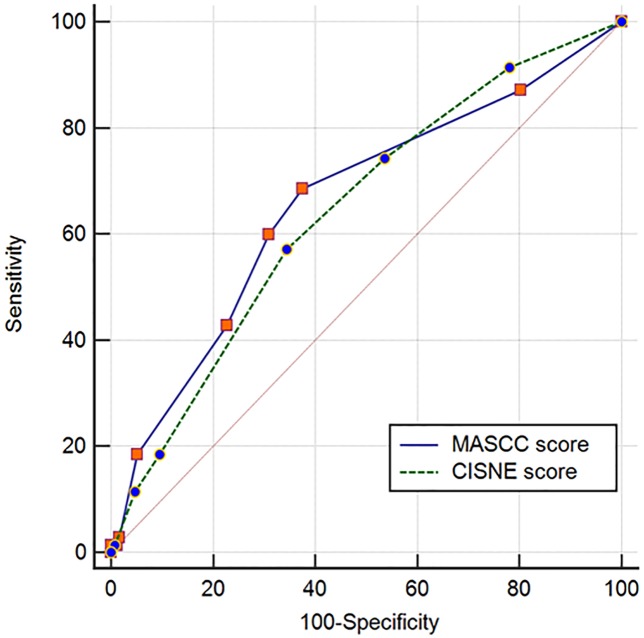
Advances in oncology have enabled physicians to treat low-risk febrile neutropenia (FN) in outpatient settings. This study was aimed to explore the usefulness of the CISNE model and identify better triage in the emergency setting. This is a retrospective cohort study on 400 adult FN patients presenting to the Emergency Department of National Cancer Center, Korea from January 2010 to December 2016. All had been treated with cytotoxic chemotherapy for solid tumors in the previous 30 days. The primary outcome was the frequency of any serious complications during the duration of illness. Apparently stable patients numbered 299 (74.8%) of 400, and the remainder comprised clinically unstable patients. The stable patients fell into three cohorts according to the risk scores: CISNE I (low risk), 56 patients (18.7%); CISNE II (intermediate), 124 (41.5%) and CISNE III (high), 119 (39.8%). The primary outcome occurred in 10.7%, 19.4% and 33.6%, respectively, according to the cohort. Compared with the Multinational Association of Supportive Care in Cancer Risk Index Score (MASCC RIS), CISNE I stratum had significantly lower sensitivity (0.22 vs. 0.95 of MASCC low risk) but higher specificity (0.91 vs. 0.17) to predict zero occurrence of the primary outcome. The CISNE model was useful for identifying low-risk FN patients for outpatient treatment. The combination of the CISNE and MASCC RIS may help emergency physicians cope with FN more confidently.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Comparison of the MASCC and CISNE scores for identifying low-risk neutropenic fever patients: analysis of data from three emergency departments of cancer centers in three continents.Support Care Cancer. 2018 May;26(5):1465-1470. doi: 10.1007/s00520-017-3985-0. Epub 2017 Nov 22. Support Care Cancer. 2018. PMID: 29168032
-
Multinational association for supportive care in cancer (MASCC) versus clinical index of stable febrile neutropenia (CISNE): evaluation of predictive performance and clinical utility in patients with febrile neutropenia.Eur J Med Res. 2025 Aug 1;30(1):692. doi: 10.1186/s40001-025-02858-z. Eur J Med Res. 2025. PMID: 40745664 Free PMC article.
-
Application of the MASCC and CISNE Risk-Stratification Scores to Identify Low-Risk Febrile Neutropenic Patients in the Emergency Department.Ann Emerg Med. 2017 Jun;69(6):755-764. doi: 10.1016/j.annemergmed.2016.11.007. Epub 2016 Dec 29. Ann Emerg Med. 2017. PMID: 28041827
-
Accuracy of the Multinational Association of Supportive Care in Cancer (MASCC) and Clinical Index of Stable Febrile Neutropenia (CISNE) scores for predicting serious complications in adult patients with febrile neutropenia: A systematic review and meta-analysis.Crit Rev Oncol Hematol. 2020 May;149:102922. doi: 10.1016/j.critrevonc.2020.102922. Epub 2020 Mar 3. Crit Rev Oncol Hematol. 2020. PMID: 32244162
-
Current management of chemotherapy-induced neutropenia in adults: key points and new challenges: Committee of Neoplastic Supportive-Care (CONS), China Anti-Cancer Association Committee of Clinical Chemotherapy, China Anti-Cancer Association.Cancer Biol Med. 2020 Nov 15;17(4):896-909. doi: 10.20892/j.issn.2095-3941.2020.0069. Epub 2020 Dec 15. Cancer Biol Med. 2020. PMID: 33299642 Free PMC article. Review.
Cited by
-
Unravelling the Proteinopathic Engagement of α-Synuclein, Tau, and Amyloid Beta in Parkinson's Disease: Mitochondrial Collapse as a Pivotal Driver of Neurodegeneration.Neurochem Res. 2025 Apr 16;50(3):145. doi: 10.1007/s11064-025-04399-7. Neurochem Res. 2025. PMID: 40240583 Review.
-
Common misconceptions in the prognostic evaluation of clinically stable patients with febrile neutropenia and solid tumors.Clin Transl Oncol. 2019 Aug;21(8):1112-1114. doi: 10.1007/s12094-018-02020-8. Epub 2019 Jan 3. Clin Transl Oncol. 2019. PMID: 30607791 No abstract available.
-
Usefulness analysis of the 2018 ASCO/IDSA guideline for outpatient management of fever and neutropenia in adults treated for malignancy.Sci Rep. 2021 Sep 15;11(1):9048. doi: 10.1038/s41598-021-88207-6. Sci Rep. 2021. PMID: 34526516 Free PMC article.
-
Clinical prediction models for febrile neutropenia and its outcomes: a systematic review.Support Care Cancer. 2025 Jun 4;33(7):537. doi: 10.1007/s00520-025-09562-y. Support Care Cancer. 2025. PMID: 40467900 Free PMC article.
-
Evaluation of the clinical Index of Stable febrile neutropenia risk stratification system for management of febrile neutropenia in gynecologic oncology patients.Gynecol Oncol Rep. 2021 Aug 27;37:100853. doi: 10.1016/j.gore.2021.100853. eCollection 2021 Aug. Gynecol Oncol Rep. 2021. PMID: 34504931 Free PMC article.
References
-
- Klastersky J, Paesmans M, Aoun M, Georgala A, Loizidou A, Lalami Y, et al. Clinical research in febrile neutropenia in cancer patients: Past achievements and perspectives for the future. World Journal of Clinical Infectious Diseases. 2016;6(3):37 10.5495/wjcid.v6.i3.37 - DOI
-
- Malik IA, Khan WA, Aziz Z, Karim M. Self-administered antibiotic therapy for chemotherapy-induced, low-risk febrile neutropenia in patients with nonhematologic neoplasms. Clin Infect Dis. 1994;19(3):522–7. . - PubMed
-
- Gardembas-Pain M, Desablens B, Sensebe L, Lamy T, Ghandour C, Boasson M. Home treatment of febrile neutropenia: an empirical oral antibiotic regimen. Ann Oncol. 1991;2(7):485–7. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
