

Platelet transfusions and mortality in necrotizing enterocolitis
- PMID: 30597571
- PMCID: PMC6402966
- DOI: 10.1111/trf.15112
Platelet transfusions and mortality in necrotizing enterocolitis
Abstract
Background: Prior studies have suggested an association between platelet transfusions (PTXs) and worse outcomes among infants with necrotizing enterocolitis (NEC), potentially mediated by proinflammatory factors released by platelets. However, the effects of storage on platelet proinflammatory factor release and the confounding role of illness severity on NEC outcomes have not been determined.
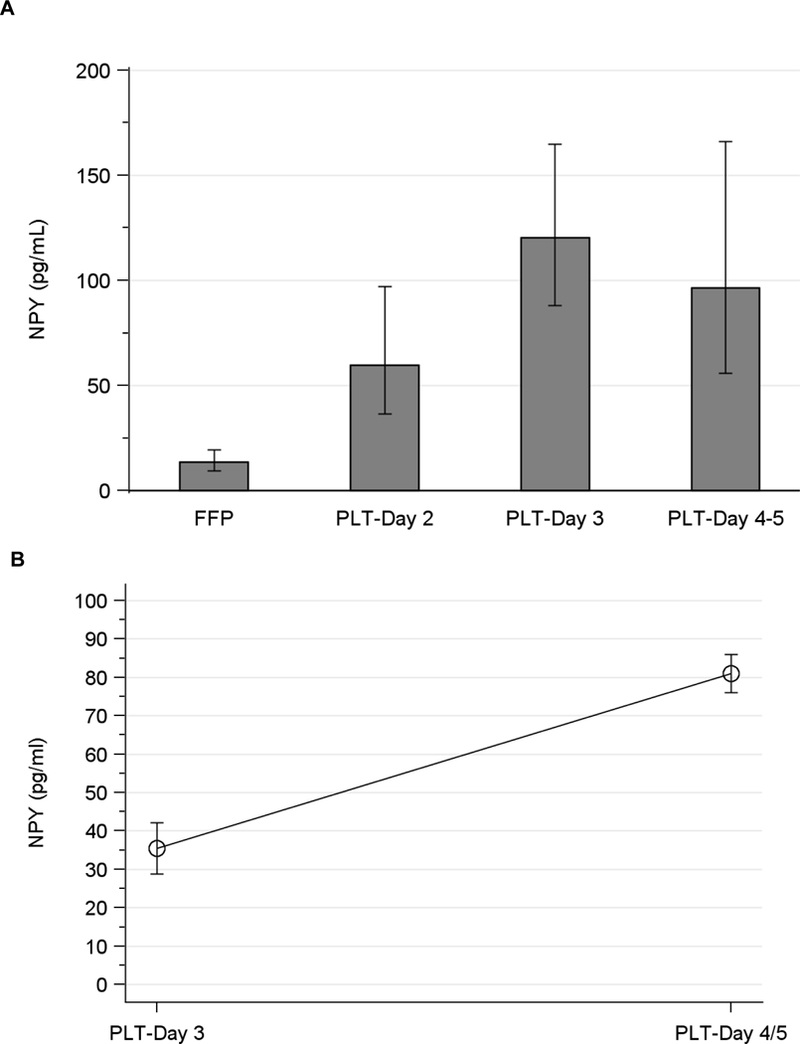
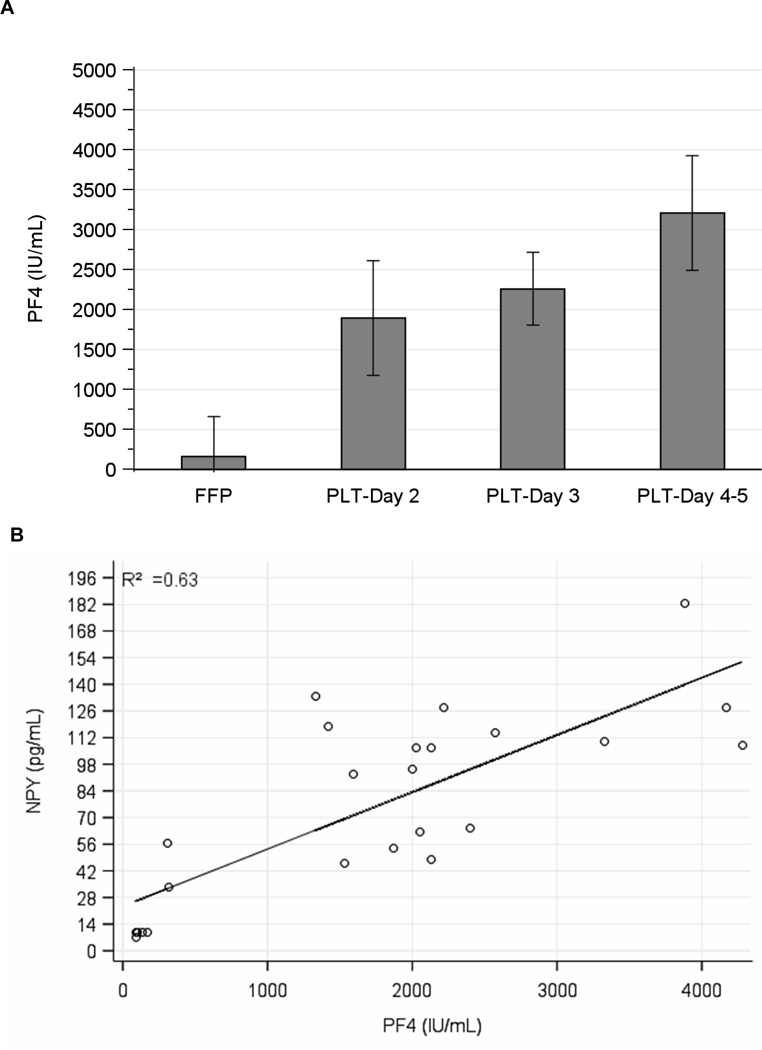
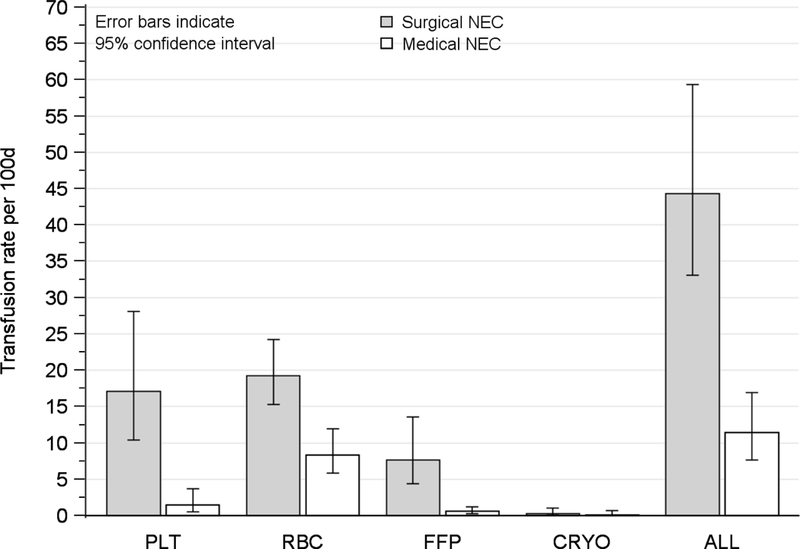
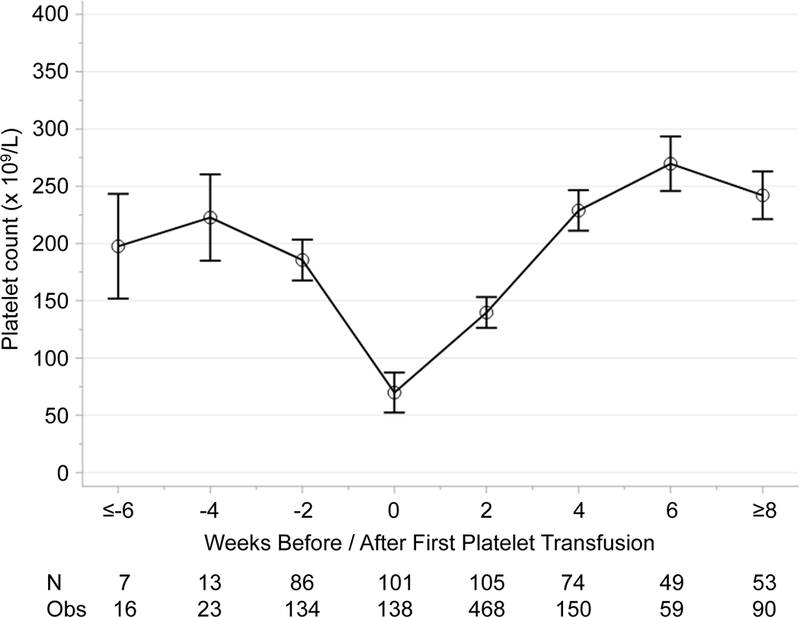
Study design and methods: First, neuropeptide Y (a potent splanchnic vasoconstrictor released by platelets) was measured by enzyme-linked immunosorbent assay in fresh frozen plasma and in the supernatant of leukoreduced apheresis-derived platelets at different times during storage. Next, we evaluated the relationship between PTX rates and death in a multicenter cohort of very-low-birth-weight infants with NEC, adjusting for illness severity.
Results: Neuropeptide Y levels increased over time in the supernatant of leukoreduced apheresis-derived platelets and were 4.4-fold and 8.9-fold higher than in fresh frozen plasma on Days 2 and 3 of storage, respectively (p < 0.001). Among 598 very-low-birth-weight infants, 44 developed NEC. In unadjusted analysis, PTX rate was 30.3 (95% confidence interval [CI], 11.5-80.1) per 100 infant-days among infants who died, compared to 6.0 (95% CI, 3.2-11.2) among survivors (incidence rate ratio, 5.1; 95% CI, 1.6-16.2; p = 0.006). In multivariable analysis, there was no association between PTX rate and mortality (incidence rate ratio, 3.0; 95% CI, 0.6-15.0; p = 0.18), although estimation was imprecise.
Conclusion: Proinflammatory mediators accumulate in platelet suspensions during storage. Although PTX rates were not associated with increased mortality among infants with NEC in our study, our estimates suggest the potential for such an association that needs evaluation in larger studies.
© 2018 AABB.
Conflict of interest statement
Figures
References
-
- Horbar JD, Edwards EM, Greenberg LT, Morrow KA, Soll RF, Buus-Frank ME, Buzas JS. Variation in Performance of Neonatal Intensive Care Units in the United States. JAMA Pediatr 2017;171: e164396. - PubMed
-
- Petrosyan M, Guner YS, Williams M, Grishin A, Ford HR. Current concepts regarding the pathogenesis of necrotizing enterocolitis. Pediatr Surg Int 2009;25: 309–18. - PubMed
-
- Baer VL, Lambert DK, Henry E, Christensen RD. Severe Thrombocytopenia in the NICU. Pediatrics 2009;124: e1095–100. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
