

Early onset cerebral amyloid angiopathy following childhood exposure to cadaveric dura
- PMID: 30597599
- PMCID: PMC6492172
- DOI: 10.1002/ana.25407
Early onset cerebral amyloid angiopathy following childhood exposure to cadaveric dura
Abstract
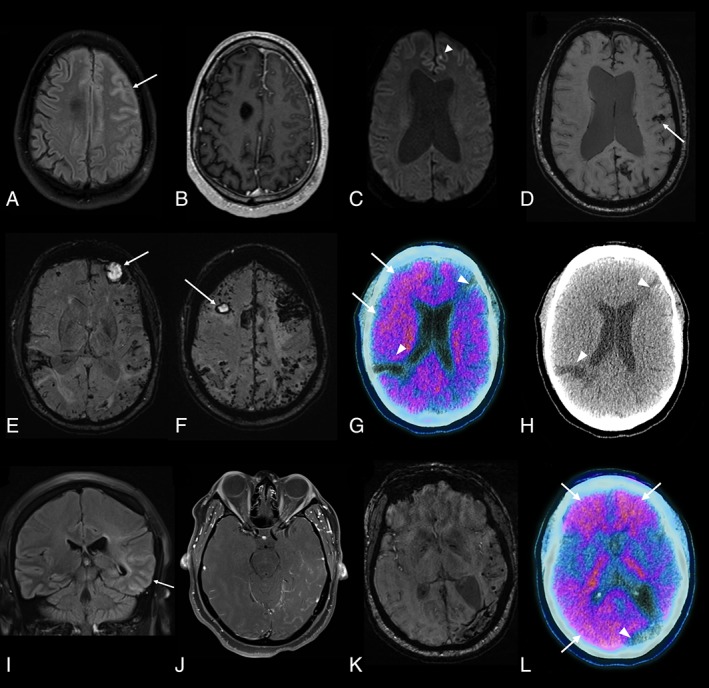
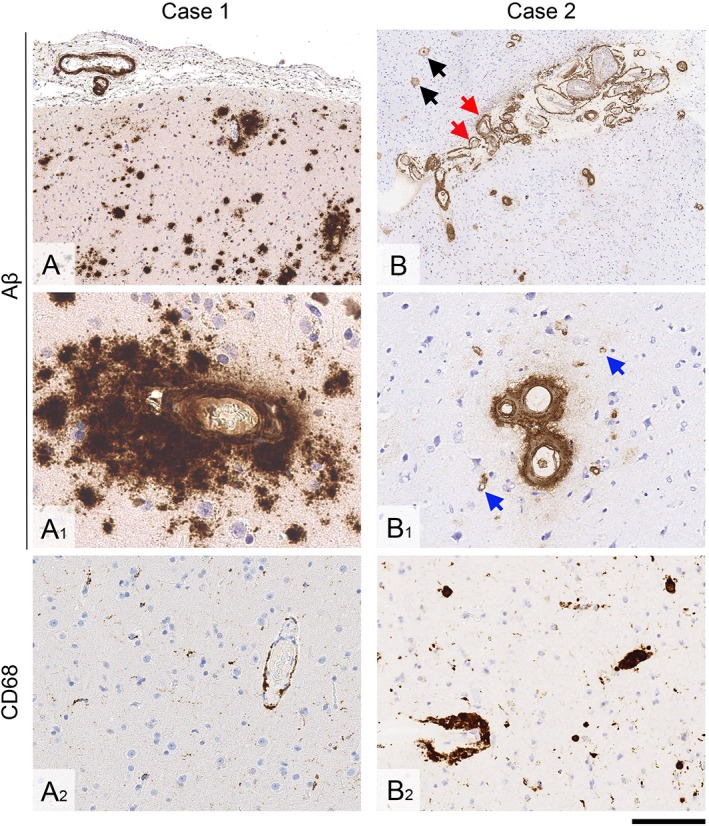
Amyloid-β transmission has been described in patients both with and without iatrogenic Creutzfeldt-Jakob disease; however, there is little information regarding the clinical impact of this acquired amyloid-β pathology during life. Here, for the first time, we describe in detail the clinical and neuroimaging findings in 3 patients with early onset symptomatic amyloid-β cerebral amyloid angiopathy following childhood exposure to cadaveric dura (by neurosurgical grafting in 2 patients and tumor embolization in a third). Our observations provide further in vivo evidence that cerebral amyloid angiopathy might be caused by transmission of amyloid-β seeds (prions) present in cadaveric dura and have diagnostic relevance for younger patients presenting with suspected cerebral amyloid angiopathy. Ann Neurol 2019; 1-7 ANN NEUROL 2019;85:284-290.
© 2018 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Conflict of interest statement
Nothing to report.
Figures
References
-
- Jaunmuktane Z, Mead S, Ellis M, et al. Evidence for human transmission of amyloid‐beta pathology and cerebral amyloid angiopathy. Nature 2015;525:247–250. - PubMed
-
- Frontzek K, Lutz MI, Aguzzi A, et al. Amyloid‐beta pathology and cerebral amyloid angiopathy are frequent in iatrogenic Creutzfeldt‐Jakob disease after dural grafting. Swiss Med Wkly 2016;146:w14287. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
