

Factors at de novo donor-specific antibody initial detection associated with allograft loss: a multicenter study
- PMID: 30597643
- PMCID: PMC6483899
- DOI: 10.1111/tri.13395
Factors at de novo donor-specific antibody initial detection associated with allograft loss: a multicenter study
Abstract
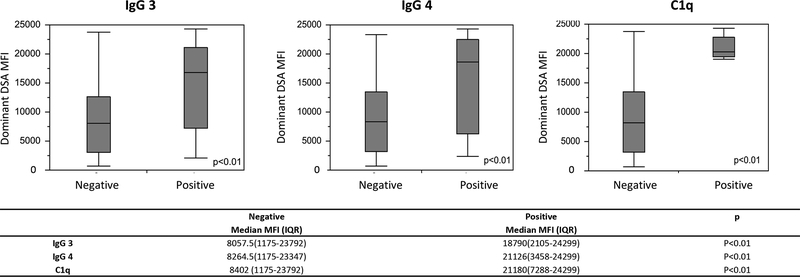
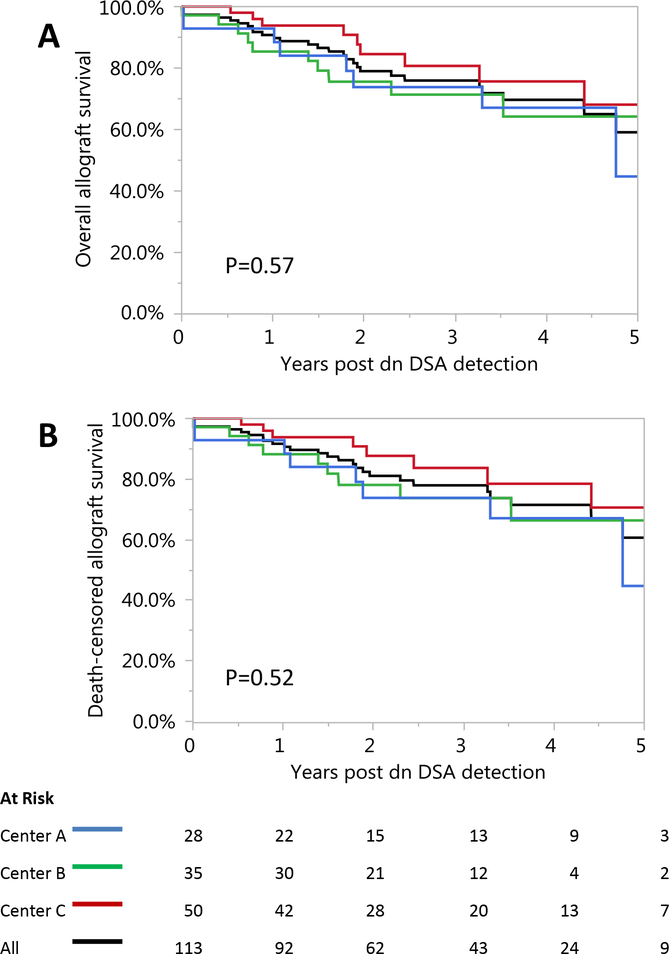
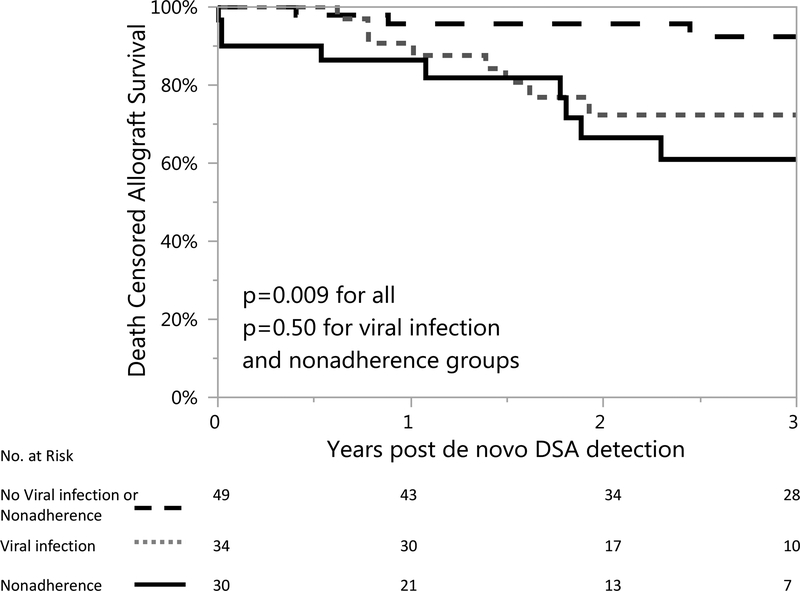
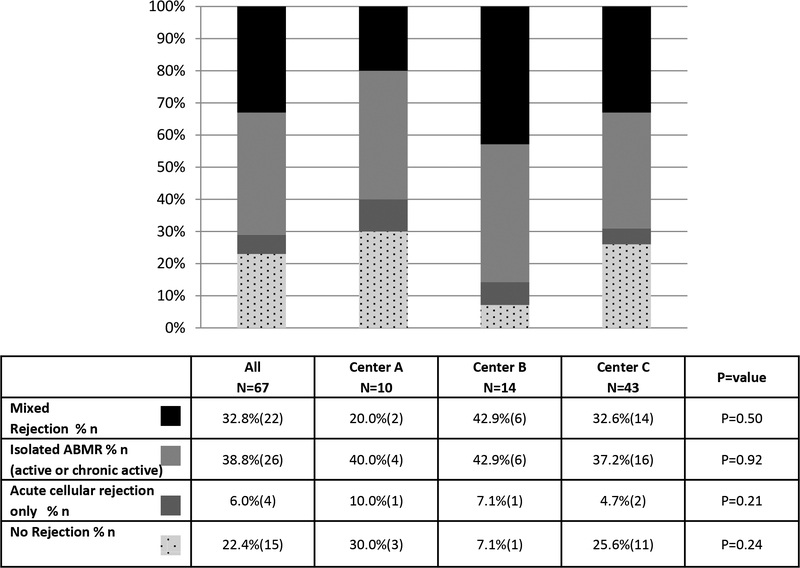
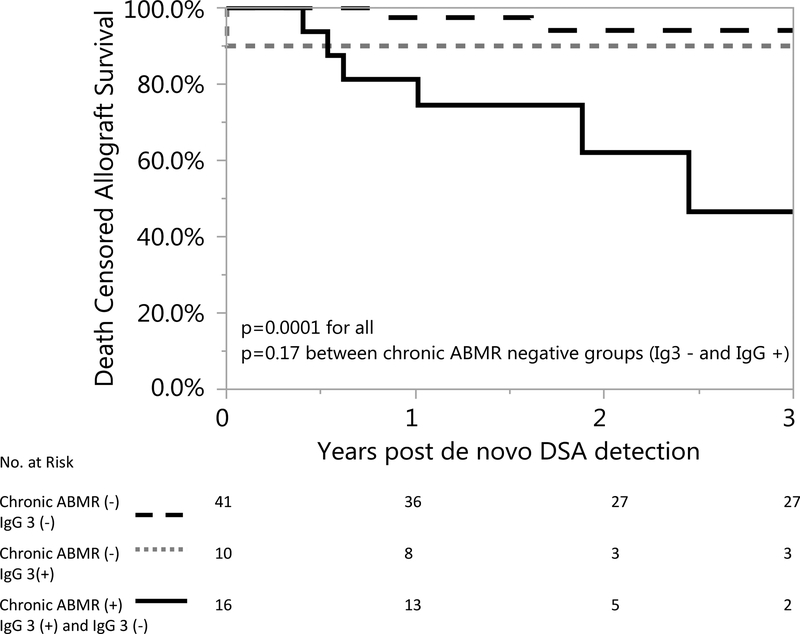
We aimed to evaluate patient factors including nonadherence and viral infection and de novo donor-specific antibody (dnDSA) characteristics [total immunoglobulin G (IgG), C1q, IgG3, and IgG4] as predictors of renal allograft failure in a multicenter cohort with dnDSA. We performed a retrospective observational study of 113 kidney transplant recipients with dnDSA and stored sera for analysis. Predictors of death-censored allograft loss were assessed by Cox proportional modeling. Death-censored allograft survival was 77.0% (87/113) during a median follow-up of 2.2 (IQR 1.2-3.7) years after dnDSA detection. Predictors of allograft failure included medication nonadherence [HR 6.5 (95% CI 2.6-15.9)], prior viral infection requiring immunosuppression reduction [HR 5.3 (95% CI 2.1-13.5)], IgG3 positivity [HR 3.8 (95% CI 1.5, 9.3)], and time post-transplant (years) until donor-specific antibody (DSA) detection [HR 1.2 (95% CI 1.0, 1.3)]. In the 67 patients who were biopsied at dnDSA detection, chronic antibody-mediated rejection [HR 11.4 (95% CI 2.3, 56.0)] and mixed rejection [HR 7.4 (95% CI 2.2, 24.8)] were associated with allograft failure. We conclude that patient factors, including a history of viral infection requiring immunosuppression reduction or medication nonadherence, combined with DSA and histologic parameters must be considered to understand the risk of allograft failure in patients with dnDSA.
Keywords: HLA-antibody post-transplantation; histocompatibility and immunogenetics; infection; kidney clinical; other; rejection.
© 2019 Steunstichting ESOT.
Conflict of interest statement
Disclosure:
The authors of this manuscript have no conflicts of interest to disclose as defined by the
Figures
References
-
- Everly MJ, Rebellato LM, Haisch CE, et al. Incidence and impact of de novo donor-specific alloantibody in primary renal allografts. Transplantation. 2013;95(3):410–417. - PubMed
-
- Cooper JE, Gralla J, Chan L, Wiseman AC. Clinical significance of post kidney transplant de novo DSA in otherwise stable grafts. Clin Transpl. 2011:359–364. - PubMed
-
- Hourmant M, Cesbron-Gautier A, Terasaki PI, et al. Frequency and clinical implications of development of donor-specific and non-donor-specific HLA antibodies after kidney transplantation. J Am Soc Nephrol. 2005;16(9):2804–2812. - PubMed
-
- Wiebe C, Gibson IW, Blydt-Hansen TD, et al. Evolution and clinical pathologic correlations of de novo donor-specific HLA antibody post kidney transplant. Am J Transplant. 2012;12(5):1157–1167. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
