

Hellenic Association for the Study of the Liver Clinical Practice Guidelines: Autoimmune hepatitis
- PMID: 30598587
- PMCID: PMC6302199
- DOI: 10.20524/aog.2018.0330
Hellenic Association for the Study of the Liver Clinical Practice Guidelines: Autoimmune hepatitis
Abstract
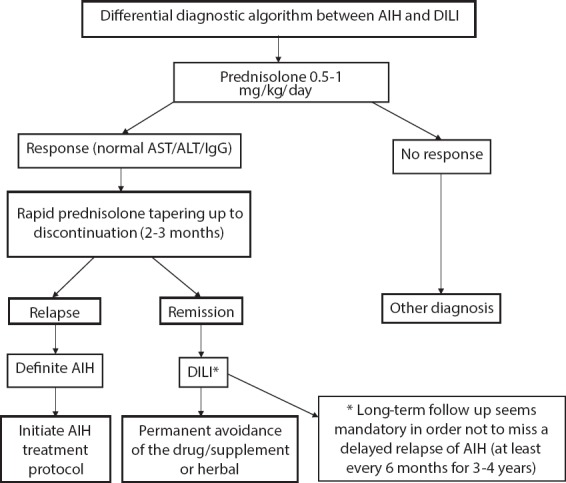
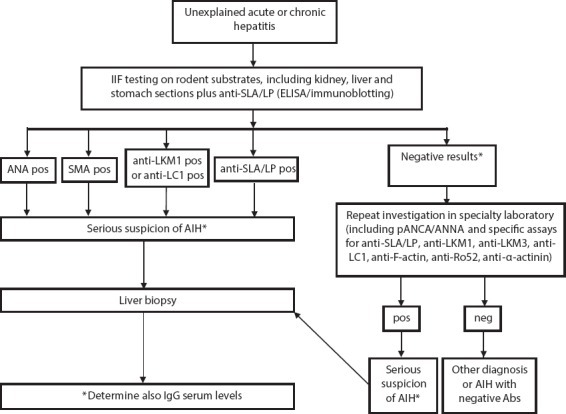
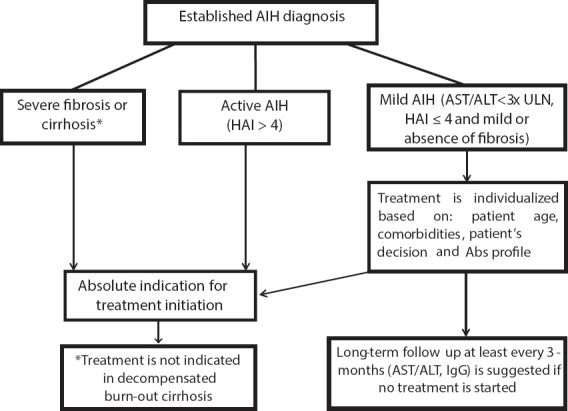
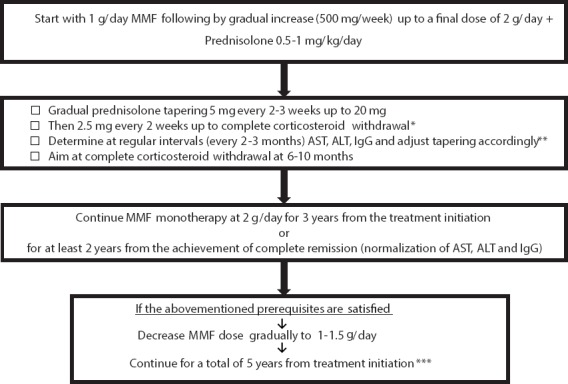
Autoimmune hepatitis (AIH) is a relatively rare acute or chronic liver disease of unknown etiology characterized by large heterogeneity. Its distribution is global, covering all ages, both sexes and all ethnic groups. The aim of the present Clinical Practice Guidelines (CPG) of the Hellenic Association for the Study of the Liver was to provide updated guidance and help to gastroenterologists, hepatologists, internists and general practitioners for AIH diagnosis and management. AIH diagnosis is based on clinicopathological characteristics: namely, polyclonal hypergammaglobulinemia, particularly of immunoglobulin G (IgG), circulating autoantibodies, interface hepatitis on liver histology, absence of viral hepatitis, and a favorable response to immunosuppression. Clinical manifestations at disease onset are variable, ranging from asymptomatic to the acute/severe form. Aminotransferase and bilirubin levels vary, while the presence of hepatitis at the histological level is a prerequisite for diagnosis. Autoantibodies are the hallmark for AIH diagnosis; therefore, the CPG describe the appropriate serological algorithm for their detection. AIH therapy should aim to achieve complete biochemical (normalization of IgG and aminotransferases) and histological remission. All patients who have active disease, even those with cirrhosis, should be treated with individualized and response-guided induction therapy using prednisolone in combination with azathioprine or mycophenolate mofetil as first-line therapy. Immunosuppression should be given for at least 3 years and for at least 2 years after the achievement of complete biochemical response, while a liver biopsy should be recommended before treatment discontinuation. Current CPG are also provided for several specific conditions and difficult-to-treat patients.
Keywords: Autoimmune hepatitis; autoantibodies; azathioprine; clinical practice guidelines; corticosteroids.
Conflict of interest statement
Conflict of Interest: None.
Figures
References
-
- Waldenström J. Leber. Blutproteine und Nahrungseiweiss. Deutsch Z Verdau Stoffwechselkr. 1950;15:113–119. - PubMed
-
- Cowling DC, Mackay IR, Taft LI. Lupoid hepatitis. Lancet. 1956;268:1323–1326. - PubMed
-
- Mackay IR, Weiden S, Hasker J. Autoimmune hepatitis. Ann NY Acad Sci. 1965;124:767–780. - PubMed
-
- Johnson PJ, McFarlane IG. Meeting report:International Autoimmune Hepatitis Group. Hepatology. 1993;18:998–1005. - PubMed
-
- Shaneyfelt TM, Mayo-Smith MF, Rothwangl J. Are guidelines following guidelines?The methodological quality of clinical practice guidelines in the peer-reviewed medical literature. JAMA. 1999;281:1900–1905. - PubMed
LinkOut - more resources
Full Text Sources