

Editorial
doi: 10.21037/qims.2018.11.09.
Pediatric stroke: current diagnostic and management challenges
Affiliations
- PMID: 30598876
- PMCID: PMC6288056
- DOI: 10.21037/qims.2018.11.09
Item in Clipboard
Editorial
Pediatric stroke: current diagnostic and management challenges
Quant Imaging Med Surg.
2018 Nov.
No abstract available
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
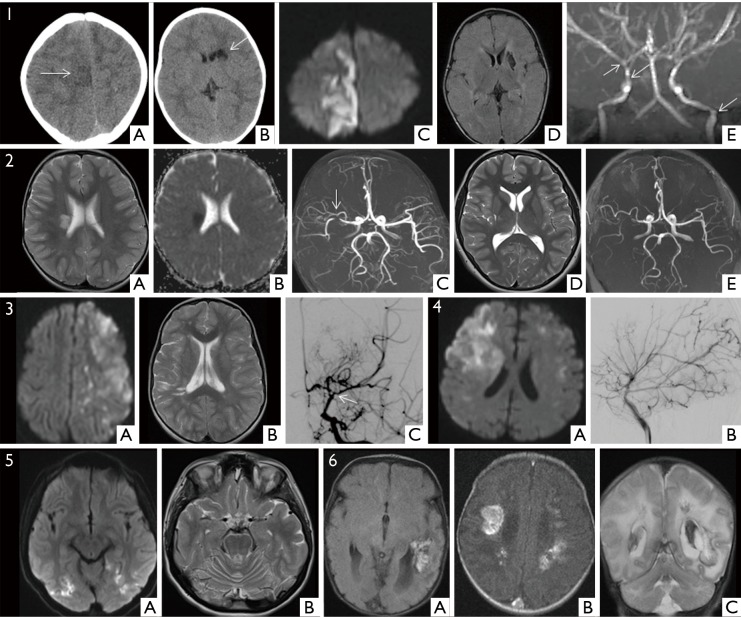
Pediatric stroke has diverse etiopathogenesis. One size does not fit all! Case 1: Fibromuscular dysplasia. A 14-month-old boy presenting with 3 episodes of acute focal seizures of his left face, arm and leg without loss of consciousness and with residual left hemiplegia. Non-contrast CT showed low attenuation lesion in the right parasagittal cortex consistent with an acute infarct (arrow) (1A). It also showed a chronic cavitated infarct in the left caudate nucleus (arrow) (1B). Diffusion weighted imaging (1C) confirmed right anterior cerebral artery acute infarct; FLAIR imaging confirmed chronic left basal ganglia infarct (1D); MRA showed beading appearance of vessels (arrows) (1E). Case 2: Focal cerebral arteriopathy (FCA). A 5-year-old girl with acute onset of left sided weakness following chicken pox infection 5 weeks previously. T2 weighted (2A) and ADC (2B) revealed acute infarct in the right corona radiata with focal stenosis of the right MCA on the MRA (arrow) (2C). Follow up imaging 10 years later (2D and 2E) shows a mature focal infarct but stable angiographic findings. Case 3: Moyamoya disease. Arterial ischemic strokes of variable ages in a 7-year-old girl with sickle cell disease shown on the DWI and T2 weighted images (3A,3B). Digital Subtraction Angiogram (DSA) (3C) confirms occlusive arteriopathy of the internal carotid T-junction (arrow) with extensive typically described ‘puff of smoke’ basal collateralization. Case 4: ACTA 2 mutation. A 6-year-old boy showing the typical imaging phenotype of ACTA 2 related stroke, a mixture of acute and chronic infarcts (4A), proximal dilatation of the large arteries (4B) with terminal tapering and smooth peripheral arteries (branches of a tree appearance). Note the absence of basal collaterals. ACTA 2 is a mutation affecting the smooth muscle alpha-actin complex. Case 5: Mitochondrial encephalopathy with lactic acidosis and stroke like episodes (MELAS). A 16-year-old girl with acute infarcts in multiple areas of the brain shown on DWI (5A) not confirming to vascular territories, and cerebellar atrophy (5B), consistent with a mitochondrial stroke pattern. The MR angiogram was normal. Case 6: Hemorrhagic venous infarction. A 25-day-old term neonate presenting with seizures. Extensive venous hemorrhagic infarction is noted in both cerebral hemispheres, particularly involving the trans-medullary veins (6A,6B,6C). The CSF tested positive for parechovirus infection. Sepsis is a common cause of infarction in the very young children.
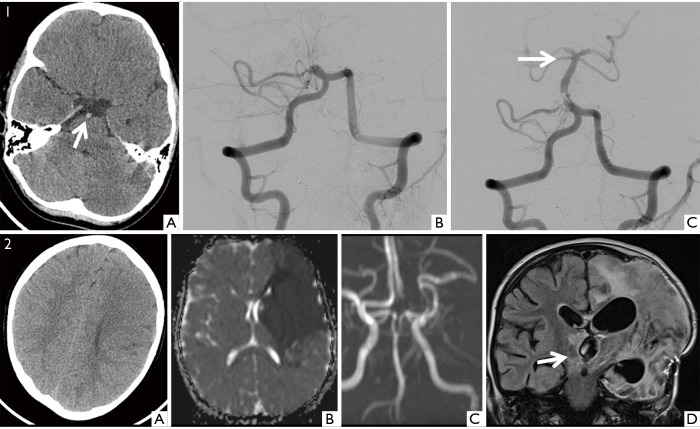
Acute management of stroke in children needs to be evaluated on a case by case basis. Case 1: Mechanical thrombectomy. A 5-year-old boy suffering from a diarrhoeal illness presented with acute loss of consciousness. He was intubated and an unenhanced CT scan was performed, showing a dense basilar artery (arrow) (1A). The patient was transferred to the regional stroke centre within an hour. DSA performed 3 hours after onset of symptoms confirmed occlusion of the basilar artery (1B). The clot was mechanically retrieved with a 4×20 mm2 Solitaire stent. Post intervention angiogram revealed recanalization (arrow) (1C). There was some hind brain swelling that needed surgical posterior fossa decompression, but no neurological deficits followed. Case 2: Large infarction needing decompression. This 5-year-old boy had a large left MCA territory infarction. Initial CT scan (2A) was performed 3 hours after onset of signs. Diffusion MR (2B) was performed 3 further hours later confirming the large infarct and lack of signal in the left MCA due to a proximal occlusion (2C). Salvageable brain tissue could not be confirmed. The patient went on to develop brain swelling needing decompression craniectomy on day 5 (2D), by which time the contralateral posterior circulation was already infarcted (arrow). Brain swelling increases from day 2 onwards and often the contralateral posterior cerebral artery is secondarily compressed against the tent as the hemisphere swells in such cases.
References
-
- RCPCH. Stroke in childhood - clinical guideline for diagnosis, management and rehabilitation | RCPCH. Royal College of Paediatrics and Child Health; 2017.
Publication types
LinkOut - more resources
Full Text Sources