

Are Porphyromonas gingivalis Outer Membrane Vesicles Microbullets for Sporadic Alzheimer's Disease Manifestation?
- PMID: 30599043
- PMCID: PMC6311351
- DOI: 10.3233/ADR-180080
Are Porphyromonas gingivalis Outer Membrane Vesicles Microbullets for Sporadic Alzheimer's Disease Manifestation?
Abstract
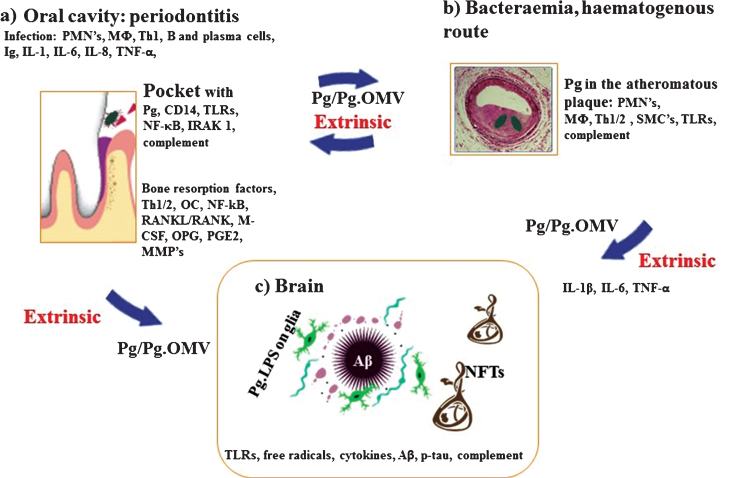
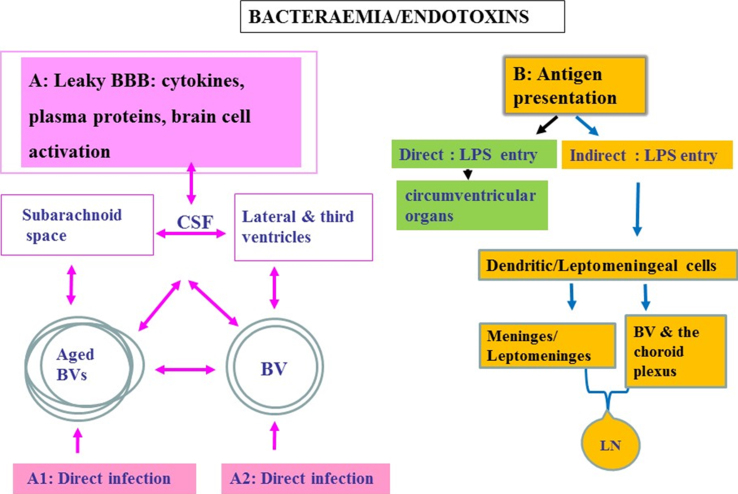
Our research into Alzheimer's disease (AD) focuses on the oral cavity and the brain, from which key evaluations of prospective and retrospective population-based data have shown that chronic periodontal disease existing for ten-years or over doubles the risk for the sporadic form of AD. Furthermore, Porphyromonas gingivalis (P. gingivalis) mono-infections in established periodontal lesions, or introducing its lipopolysachharide (LPS), as demonstrated in in vivo studies, show hallmark pathology inclusive of extracellular amyloid plaques and phospho-tau bound neurofibrillary tangles with AD-like phenotype. Other studies have shown that if periodontitis remains untreated in human AD patients, cognitive decline ensues. This is a bi-directional relationship meaning that the converse is also true; treating periodontal disease in AD patients improves memory. Bacterial cultures and established oral biofilms generate vast numbers of microvesicles and P. gingivalis outer membrane vesicles encase key virulence factors (LPS, gingipains, capsule, fimbriae) as though they are complete destructive "microbullets" when shed in the host. This provides P. gingivalis additional arsenal to manipulate its entry into disparate organs, hijack phagocytosis, destroy tissues, and affect complement related genes while transducing the onset of proinflammatory signaling cascades. The resulting inflammatory mediators may be the cause of disease defining lesions and cognitive decline typical of clinical AD.
Keywords: Alzheimer’s disease; P. gingivalis; microbullets; outer membrane vesicles; periodontitis.
Figures
Similar articles
-
Assessing the role of Porphyromonas gingivalis in periodontitis to determine a causative relationship with Alzheimer's disease.J Oral Microbiol. 2019 Jan 29;11(1):1563405. doi: 10.1080/20002297.2018.1563405. eCollection 2019. J Oral Microbiol. 2019. PMID: 30728914 Free PMC article. Review.
-
Porphyromonas gingivalis is a Strong Risk Factor for Alzheimer's Disease.J Alzheimers Dis Rep. 2020 Dec 14;4(1):501-511. doi: 10.3233/ADR-200250. J Alzheimers Dis Rep. 2020. PMID: 33532698 Free PMC article. Review.
-
Alzheimer's Disease and Porphyromonas gingivalis: Exploring the Links.Life (Basel). 2025 Jan 14;15(1):96. doi: 10.3390/life15010096. Life (Basel). 2025. PMID: 39860036 Free PMC article. Review.
-
Oral Porphyromonas gingivalis Infections Increase the Risk of Alzheimer's Disease: A Review.Oral Health Prev Dent. 2023 Jan 18;21:7-16. doi: 10.3290/j.ohpd.b3818045. Oral Health Prev Dent. 2023. PMID: 36651311 Free PMC article. Review.
-
Periodontitis as a Risk Factor for Alzheimer's Disease: The Experimental Journey So Far, with Hope of Therapy.Adv Exp Med Biol. 2022;1373:241-260. doi: 10.1007/978-3-030-96881-6_13. Adv Exp Med Biol. 2022. PMID: 35612802
Cited by
-
Membrane Vesicles Derived from Gut Microbiota and Probiotics: Cutting-Edge Therapeutic Approaches for Multidrug-Resistant Superbugs Linked to Neurological Anomalies.Pharmaceutics. 2022 Nov 3;14(11):2370. doi: 10.3390/pharmaceutics14112370. Pharmaceutics. 2022. PMID: 36365188 Free PMC article. Review.
-
Porphyromonas gingivalis Conditioned Medium Induces Amyloidogenic Processing of the Amyloid-β Protein Precursor upon in vitro Infection of SH-SY5Y Cells.J Alzheimers Dis Rep. 2022 Sep 20;6(1):577-587. doi: 10.3233/ADR-220029. eCollection 2022. J Alzheimers Dis Rep. 2022. PMID: 36275415 Free PMC article.
-
Do Oral Pathogens Inhabit the Eye and Play a Role in Ocular Diseases?J Clin Med. 2022 May 23;11(10):2938. doi: 10.3390/jcm11102938. J Clin Med. 2022. PMID: 35629064 Free PMC article. Review.
-
Outer membrane vesicles of Porphyromonas gingivalis: recent advances in pathogenicity and associated mechanisms.Front Microbiol. 2025 Apr 1;16:1555868. doi: 10.3389/fmicb.2025.1555868. eCollection 2025. Front Microbiol. 2025. PMID: 40256625 Free PMC article. Review.
-
Antibodies with specificity to glycan motifs that decorate OMV cargo proteins.mSphere. 2025 Mar 25;10(3):e0090724. doi: 10.1128/msphere.00907-24. Epub 2025 Feb 26. mSphere. 2025. PMID: 40008882 Free PMC article.
References
-
- Olsen I (2008) Update on bacteraemia related to dental procedures. Transfus Apher Sci 39, 173–178. - PubMed
-
- Tzeng NS, Chung CH, Yeh CB, Huang RY, Yuh DY, Huang SY, Lu RB, Chang HA, Kao YC, Chiang WS, Chou YC, Chien WC (2016) Are chronic periodontitis and gingivitis associated with dementia? A nationwide, retrospective, matched-cohort study in Taiwan. Neuroepidemiology 47, 82–93. - PubMed
LinkOut - more resources
Full Text Sources
