

Improvements in treatment planning calculations motivated by tightening IMRT QA tolerances
- PMID: 30599085
- PMCID: PMC6333129
- DOI: 10.1002/acm2.12524
Improvements in treatment planning calculations motivated by tightening IMRT QA tolerances
Abstract
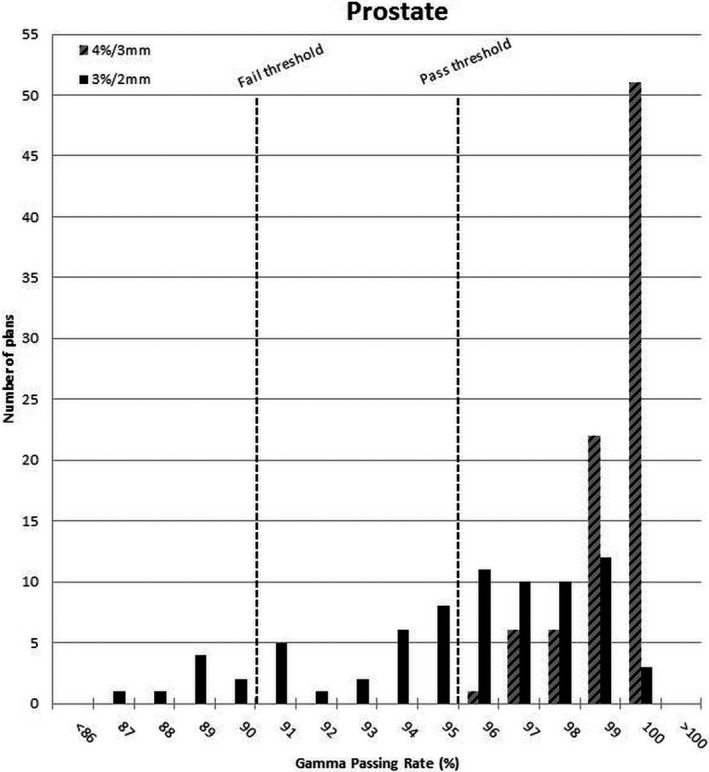
Implementing tighter intensity modulated radiation therapy (IMRT) quality assurance (QA) tolerances initially resulted in high numbers of marginal or failing QA results and motivated a number of improvements to our calculational processes. This work details those improvements and their effect on results. One hundred eighty IMRT plans analyzed previously were collected and new gamma criteria were applied and compared to the original results. The results were used to obtain an estimate for the number of plans that would require additional dose volume histogram (DVH)-based analysis and therefore predicted workload increase. For 2 months and 133 plans, the established criteria were continued while the new criteria were applied and tracked in parallel. Because the number of marginal or failing plans far exceeded the predicted levels, a number of calculational elements were investigated: IMRT modeling parameters, calculation grid size, and couch top modeling. After improvements to these elements, the new criteria were clinically implemented and the frequency of passing, questionable, and failing plans measured for the subsequent 15 months and 674 plans. The retrospective analysis of selected IMRT QA results demonstrated that 75% of plans should pass, while 19% of IMRT QA plans would need DVH-based analysis and an additional 6% would fail. However, after applying the tighter criteria for 2 months, the distribution of plans was significantly different from prediction with questionable or failing plans reaching 47%. After investigating and improving several elements of the IMRT calculation processes, the frequency of questionable plans was reduced to 11% and that of failing plans to less than 1%. Tighter IMRT QA tolerances revealed the need to improve several elements of our plan calculations. As a consequence, the accuracy of our plans have improved, and the frequency of finding marginal or failing IMRT QA results, remains within our practical ability to respond.
Keywords: IMRT QA; patient-specific QA; treatment planning systems.
© 2018 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Figures





Similar articles
-
A clinically relevant IMRT QA workflow: Design and validation.Med Phys. 2018 Apr;45(4):1391-1399. doi: 10.1002/mp.12838. Epub 2018 Mar 23. Med Phys. 2018. PMID: 29481698
-
Institutional patient-specific IMRT QA does not predict unacceptable plan delivery.Int J Radiat Oncol Biol Phys. 2014 Dec 1;90(5):1195-201. doi: 10.1016/j.ijrobp.2014.08.334. Epub 2014 Oct 21. Int J Radiat Oncol Biol Phys. 2014. PMID: 25442044 Free PMC article.
-
A method to reconstruct and apply 3D primary fluence for treatment delivery verification.J Appl Clin Med Phys. 2017 Jan;18(1):128-138. doi: 10.1002/acm2.12017. Epub 2016 Dec 8. J Appl Clin Med Phys. 2017. PMID: 28291913 Free PMC article.
-
Utilising the Virtual Environment for Radiotherapy Training System to Support Undergraduate Teaching of IMRT, VMAT, DCAT Treatment Planning, and QA Concepts.J Med Imaging Radiat Sci. 2018 Mar;49(1):31-38. doi: 10.1016/j.jmir.2017.11.002. Epub 2018 Jan 3. J Med Imaging Radiat Sci. 2018. PMID: 30479285 Review.
-
Tolerance limits and methodologies for IMRT measurement-based verification QA: Recommendations of AAPM Task Group No. 218.Med Phys. 2018 Apr;45(4):e53-e83. doi: 10.1002/mp.12810. Epub 2018 Mar 23. Med Phys. 2018. PMID: 29443390 Review.
References
-
- Stasi M, Bresciani S, Miranti A, Maggio A, Sapino V, Gabriele P. Pretreatment patient‐specific IMRT quality assurance: a correlation study between gamma index and patient clinical dose volume histogram. Med Phys. 2012;39:7626–7634. - PubMed
-
- Miften M, Olch A, Mihailidis D, et al. Tolerance limits and methodologies for IMRT measurement‐based verification QA: recommendations of AAPM Task Group No. 218. Med Phys. 2018;45:53–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
