

The Effectiveness of Noninvasive Positive Pressure Ventilation in Subarachnoid Pleural Fistula: A Case Report and Literature Review
- PMID: 30599490
- PMCID: PMC6347350
- DOI: 10.14245/ns.1836056.028
The Effectiveness of Noninvasive Positive Pressure Ventilation in Subarachnoid Pleural Fistula: A Case Report and Literature Review
Abstract
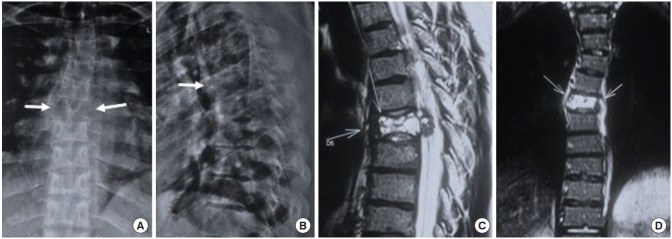
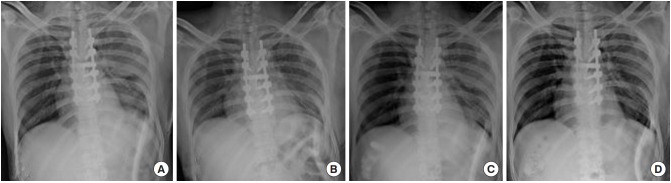
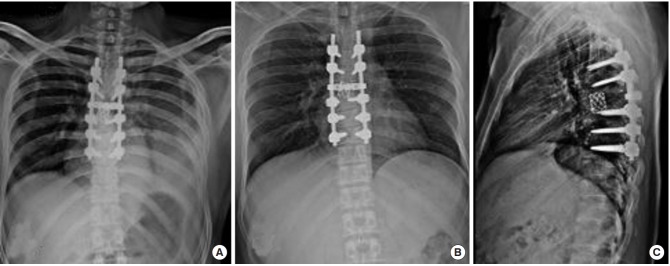
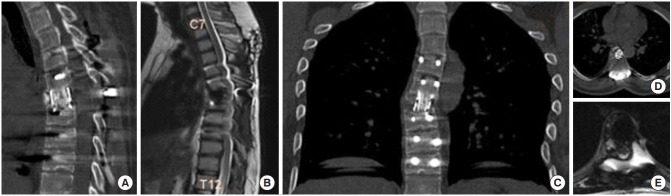
Subarachnoid pleural fistula (SPF) is an aberrant communication between the pleural cavity and subarachnoid space, resulting in uncontrolled cerebrospinal fluid drainage. The negative pressure of the pleural cavity creates a continuous suctioning effect, thereby impeding the spontaneous closure of these fistulas. Dural tears or punctures in cardiothoracic procedures, spinal operations, and trauma are known to cause such abnormal communications. Failure to recognize this entity may result in sudden neurological or respiratory complications. Hence, a high index of suspicion is required for early diagnosis and prompt management. Noninvasive positive pressure ventilation has been described to be effective in managing such fistulas, thus mitigating the high morbidity associated with exploratory surgery for primary repair. Herein, we describe the typical presentation of SPF and the clinical course, treatment, and follow-up of a patient who sustained SPF following anterior thoracic spinal surgery.
Keywords: Incidental dural tear; Noninvasive positive pressure ventilation; Subarachnoid pleural fistula.
Conflict of interest statement
The authors have nothing to disclose.
Figures


References
-
- Fountas KN, Kapsalaki EZ, Johnston KW. Cerebrospinal fluid fistula secondary to dural tear in anterior cervical discectomy and fusion: case report. Spine (Phila Pa 1976) 2005;30:E277–80. - PubMed
-
- Milloy FJ, Correll NO, Langston HT. Persistent subarachnoid-pleural space fistula; report of a case. J Am Med Assoc. 1959;169:1467. - PubMed
-
- D'Souza R, Doshi A, Bhojraj S, et al. Massive pleural effusion as the presenting feature of a subarachnoid-pleural fistula. Respiration. 2002;69:96–9. - PubMed
-
- Assietti R, Kibble MB, Bakay RA. Iatrogenic cerebrospinal fluid fistula to the pleural cavity: case report and literature review. Neurosurgery. 1993;33:1104–8. - PubMed
LinkOut - more resources
Full Text Sources
