

Pediatric cystic diseases of the kidney
- PMID: 30600488
- PMCID: PMC6704226
- DOI: 10.1007/s40477-018-0347-9
Pediatric cystic diseases of the kidney
Abstract
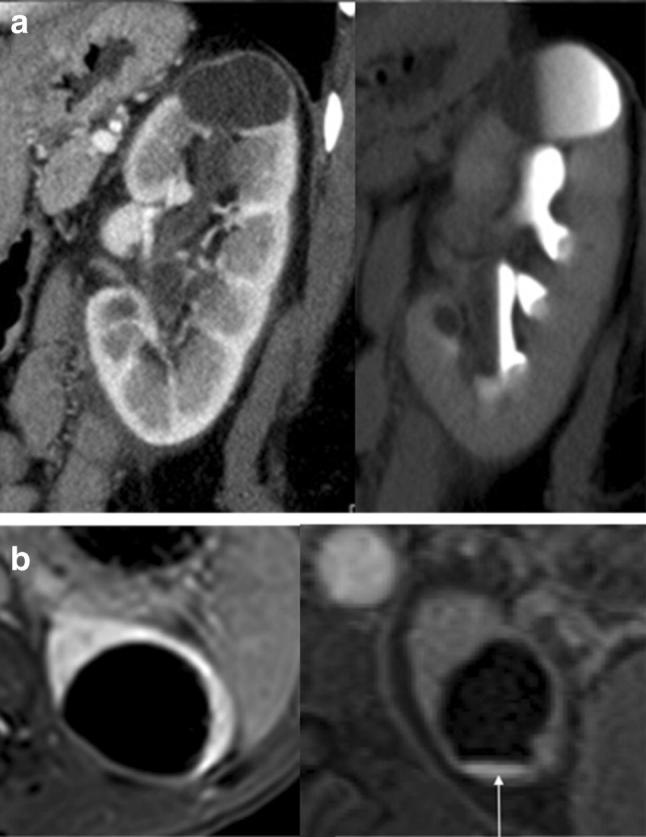
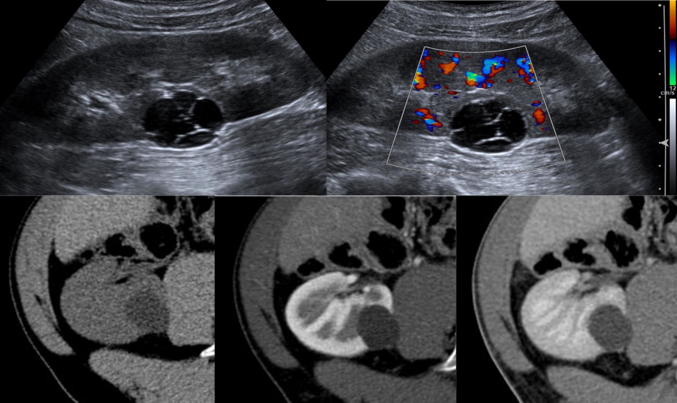
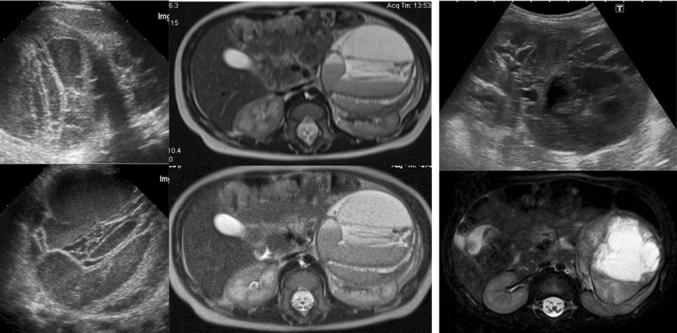
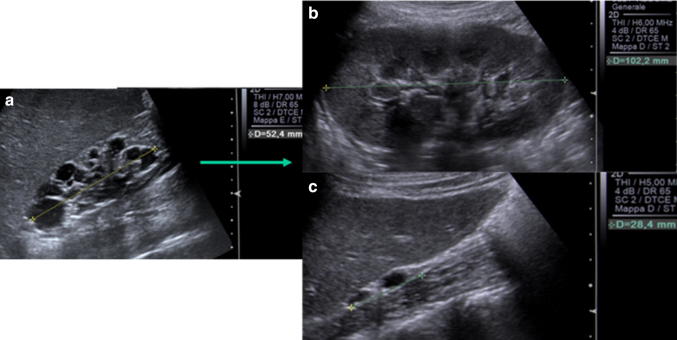
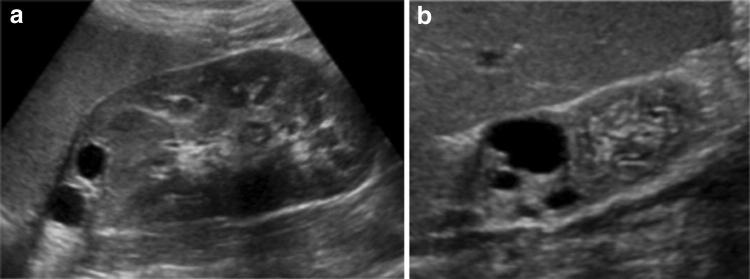
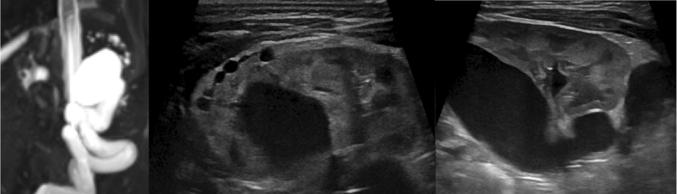
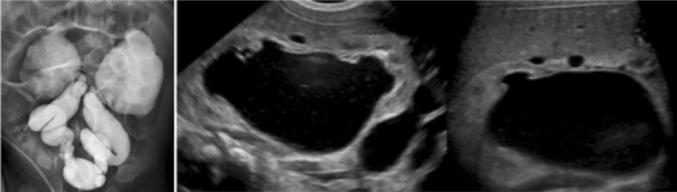
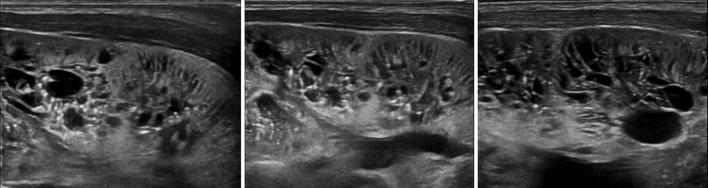
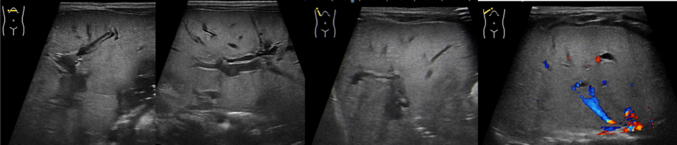
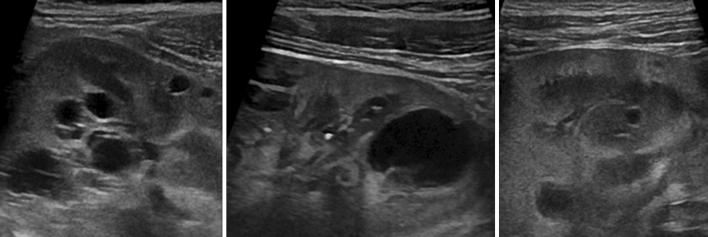
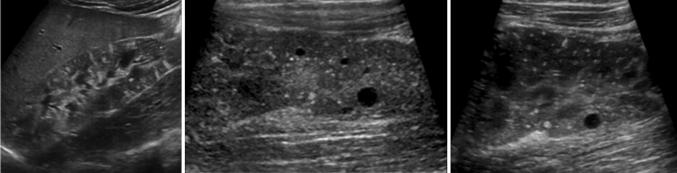
Pediatric renal cystic diseases include a variety of hereditary or non-hereditary conditions. Numerous classifications exist and new data are continuously published. Ultrasound is the primary technique for evaluating kidneys in children: conventional and high-resolution US allows a detailed visualization of renal parenchyma and of number, size and location of the cysts, hence representing the most important diagnostic imaging technique for the first diagnosis and follow-up of these young patients. The purpose of this pictorial essay is to review the spectrum of renal cystic lesions in children from simple, complex or malignant single cysts to the several poly/multicystic kidney diseases.
La patologia cistica renale in età pediatrica è costituita da svariate condizioni ereditarie e non. La letteratura propone diverse classificazioni, in continua evoluzione. L’ecografia rappresenta la prima metodica per la valutazione del rene nel neonato e nel bambino: l’esame con metodica tradizionale e con sonde ad alta risoluzione consente uno studio dettagliato del parenchima renale e delle cisti per numero, dimensioni e localizzazione. L’ecografia è pertanto il cardine nell’iter diagnostico e nel follow-up di questi piccoli pazienti. Obiettivo di questo lavoro è rivedere le peculiarità delle lesioni cistiche renali in età pediatrica: dalla cisti singola, semplice o complessa, allo spettro delle patologie multi/policistiche.
Keywords: Cystic renal disease; Kidney; Neonatal; Pediatric; Ultrasound.
Conflict of interest statement
Author Federica Ferro declares that she has no conflict of interest. Author Norberto Vezzali declares that he has no conflict of interest. Author Evi Comploj declares that she has no conflict of interest. Author Elena Pedron declares that she has no conflict of interest. Author Marco Di Serafino declares that he has no conflict of interest. Author Francesco Esposito declares that he has no conflict of interest. Author Piernicola Pelliccia declares that he has no conflict of interest. Author Eugenio Rossi declares that he has no conflict of interest. Author Massimo Zeccolini declares that he has no conflict of interest. Author Gianfranco Vallone declares that he has no conflict of interest.
Figures





References
-
- Riccabona M, Ring E, Avni F. Imaging in renal agenesis, dysplasia, hypoplasia, and cystic diseases of the kidney. In: Riccabona M, editor. Pediatric urogenital radiology. Berlin: Springer; 2018. pp. 553–577.
-
- Gupta I, Bitzan M (2104) Cystic renal disease. In: Manual of pediatric nephrology. Springer, Berlin, pp 249–262
-
- MacRae K, Chisthi A, et al. Cystic renal disease. In: Chisti AS, et al., editors. Kidney and urinary tract disease in the newborn. Berlin: Springer; 2014. pp. 263–274.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
