

Management of Clinical T1N0M0 Esophageal Cancer
- PMID: 30600672
- PMCID: PMC6529170
- DOI: 10.5009/gnl18254
Management of Clinical T1N0M0 Esophageal Cancer
Abstract
Background/aims: Endoscopic resection is a standard treatment for stage T1a esophageal cancer, with esophagectomy or radical radiation therapy (RT) performed for stage T1b lesions. This study aimed to compare treatment outcomes of each modality for clinical stage T1 esophageal cancer.
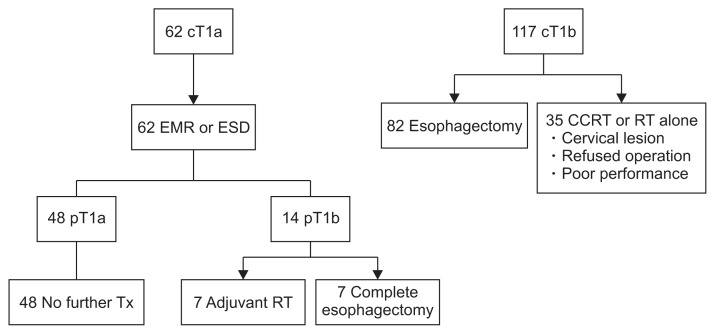
Methods: In total, 179 patients with clinical T1N0M0-stage esophageal cancer treated from 2006 to 2016 were retrospectively evaluated. Sixty-two patients with clinical T1a-stage cancer underwent endoscopic resection. Among 117 patients with clinical T1b-stage cancer, 82 underwent esophagectomy, and 35 received chemoradiotherapy or RT. We compared overall survival (OS) and recurrence-free survival (RFS) rates for each treatment modality.
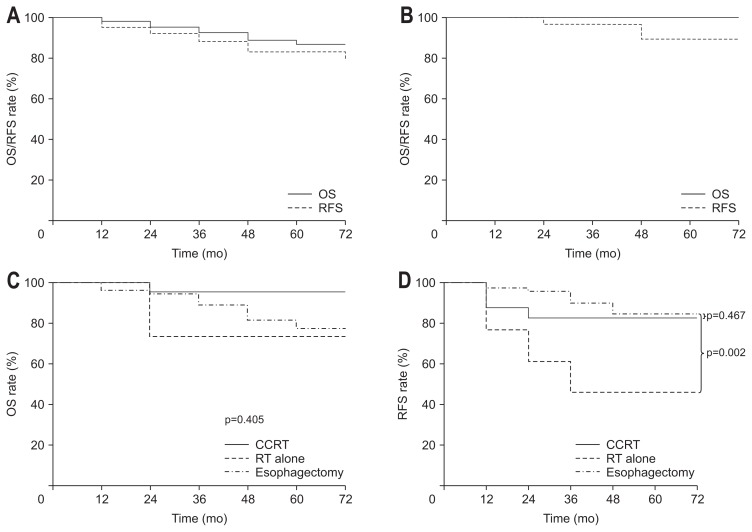
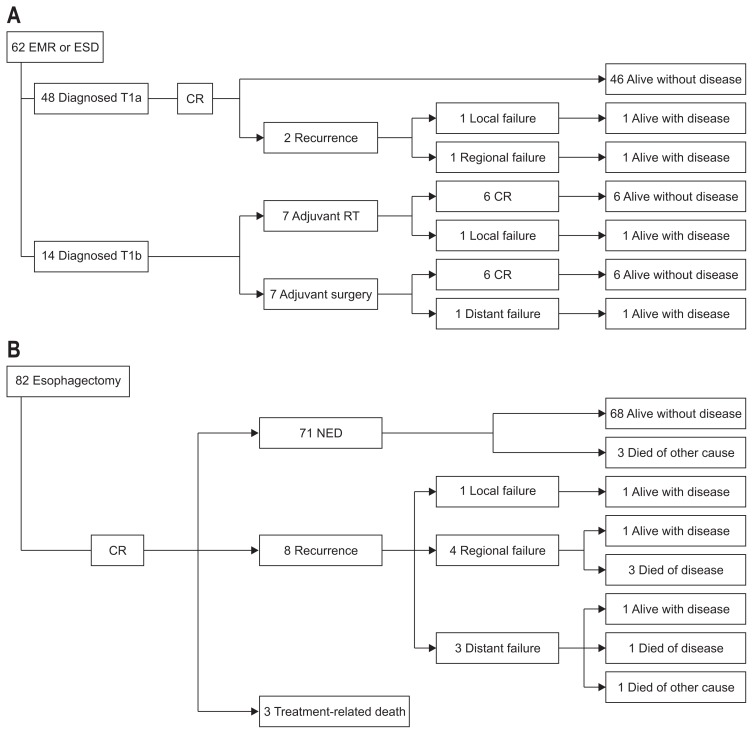
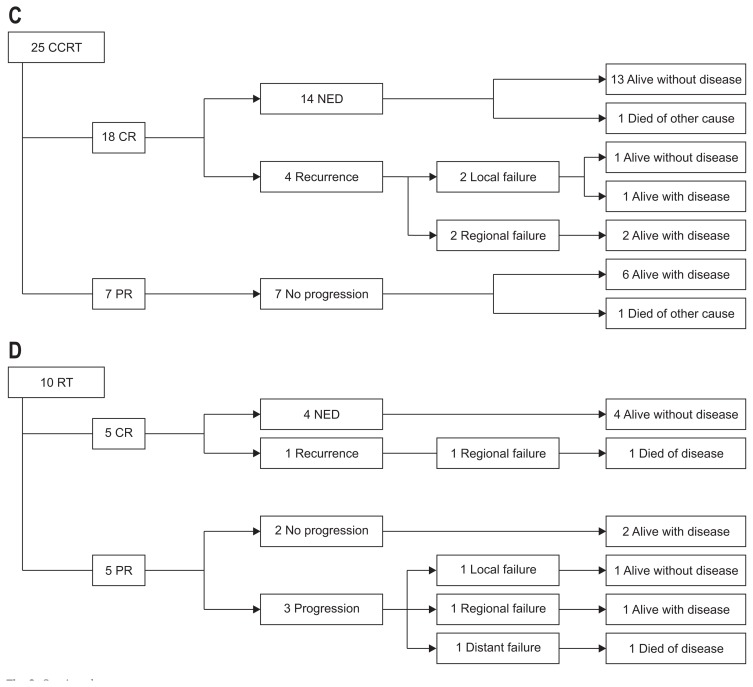
Results: The median follow-up time was 32 months (range, 1 to 120 months). The 5-year OS and RFS rates for patients with stage T1a cancer receiving endoscopic resection were 100% and 85%, respectively. For patients with stage T1b, the 5-year OS and RFS rates were 78% and 77%, respectively, for the esophagectomy group; 80% and 44%, respectively, for the RT alone group; and 96% and 80%, respectively, for the chemoradiation group. The esophagectomy group showed significantly higher RFS than the RT alone group (p=0.04). There was no significant difference in RFS between the esophagectomy and chemoradiation groups (p=0.922). Grade 4 or higher treatment-related complications occurred in four patients who underwent esophagectomy.
Conclusions: Endoscopic resection appeared to be an adequate treatment for patients with T1a-stage esophageal cancer. The multidisciplinary approach involving chemoradiation was comparable to esophagectomy in terms of survival outcome without serious complications for T1b-stage esophageal cancer.
Keywords: Chemoradiotherapy; Endoscopic mucosal resection; Esophageal neoplasm; Esophagectomy; Radiotherapy.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Endoscopic submucosal dissection followed by chemoradiotherapy for superficial esophageal cancer: choice of new approach.Radiat Oncol. 2018 Dec 14;13(1):246. doi: 10.1186/s13014-018-1195-7. Radiat Oncol. 2018. PMID: 30547811 Free PMC article.
-
Trends in Treatment of T1N0 Esophageal Cancer.Ann Surg. 2019 Sep;270(3):434-443. doi: 10.1097/SLA.0000000000003466. Ann Surg. 2019. PMID: 31274653 Free PMC article.
-
Comparison of long-term outcomes between esophagectomy and chemoradiotherapy after endoscopic resection of submucosal esophageal squamous cell carcinoma.Dis Esophagus. 2019 Dec 31;32(12):doz023. doi: 10.1093/dote/doz023. Dis Esophagus. 2019. PMID: 30980070
-
Optimal Use of Combined Modality Therapy in the Treatment of Esophageal Cancer.Surg Oncol Clin N Am. 2017 Jul;26(3):405-429. doi: 10.1016/j.soc.2017.01.009. Epub 2017 May 11. Surg Oncol Clin N Am. 2017. PMID: 28576180 Review.
-
Role of adjuvant chemoradiotherapy after endoscopic treatment of early-stage esophageal cancer: a systematic review.Minerva Chir. 2018 Aug;73(4):428-436. doi: 10.23736/S0026-4733.18.07763-5. Epub 2018 Apr 13. Minerva Chir. 2018. PMID: 29658684
Cited by
-
Risk factors for lymph node metastasis in T1 esophageal squamous cell carcinoma: A systematic review and meta-analysis.World J Gastroenterol. 2021 Feb 28;27(8):737-750. doi: 10.3748/wjg.v27.i8.737. World J Gastroenterol. 2021. PMID: 33716451 Free PMC article.
-
Long-term survival in esophagectomy for early-stage esophageal cancer versus endoscopic resection plus additional chemoradiotherapy: a systematic review and meta-analysis.J Thorac Dis. 2023 Aug 31;15(8):4387-4395. doi: 10.21037/jtd-23-376. Epub 2023 Aug 11. J Thorac Dis. 2023. PMID: 37691683 Free PMC article.
-
Comparison of Long-Term Survival Between cT1N0 Stage Esophageal Cancer Patients Receiving Endoscopic Dissection and Esophagectomy: A Meta-Analysis.Front Surg. 2022 May 6;9:917689. doi: 10.3389/fsurg.2022.917689. eCollection 2022. Front Surg. 2022. PMID: 36017523 Free PMC article.
-
Management of early oesophageal cancer: An overview.World J Gastrointest Surg. 2024 May 27;16(5):1255-1258. doi: 10.4240/wjgs.v16.i5.1255. World J Gastrointest Surg. 2024. PMID: 38817272 Free PMC article.
-
Endoscopic therapy versus esophagectomy for T1bN0M0 esophageal cancer: A population-based study using propensity score matching.Heliyon. 2023 Nov 10;9(11):e22189. doi: 10.1016/j.heliyon.2023.e22189. eCollection 2023 Nov. Heliyon. 2023. PMID: 38045191 Free PMC article.
References
-
- Rice TW, Rusch VW, Ishwaran H, Blackstone EH Worldwide Esophageal Cancer Collaboration. Cancer of the esophagus and esophagogastric junction: data-driven staging for the seventh edition of the American Joint Committee on Cancer/International Union Against Cancer Cancer Staging Manuals. Cancer. 2010;116:3763–3773. doi: 10.1002/cncr.25146. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
