

Mesenchymal Stem Cell-Based Therapies against Podocyte Damage in Diabetic Nephropathy
- PMID: 30603477
- PMCID: PMC6171601
- DOI: 10.1007/s13770-017-0026-5
Mesenchymal Stem Cell-Based Therapies against Podocyte Damage in Diabetic Nephropathy
Abstract
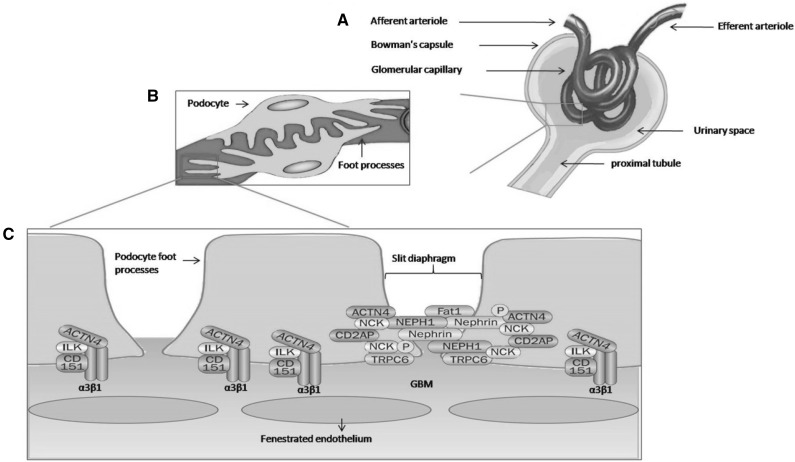
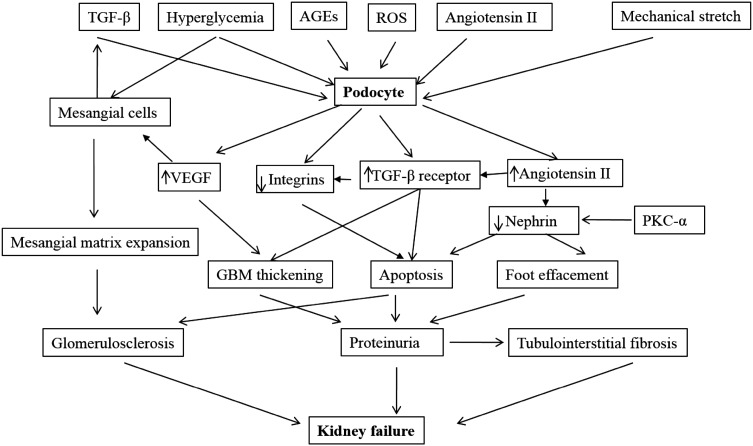
Injury to podocytes is an early event in diabetic nephropathy leading to proteinuria with possible progression to end-stage renal failure. The podocytes are unique and highly specialized cells that cover the outer layer of kidney ultra-filtration barrier and play an important role in glomerular function. In the past few decades, adult stem cells, such as mesenchymal stem cells (MSCs) with a regenerative and differentiative capacity have been extensively used in cell-based therapies. In addition to their capability for regeneration and differentiation, MSCs contributes to their milieu by paracrine action of a series of growth factors via antiapoptotic, mitogenic and other cytokine actions that actively participate in treatment of podocyte damage through prevention of podocyte effacement, detachment and apoptosis. It is hoped that novel stem cell-based therapies will be developed in the future to prevent podocyte injury, thereby reducing the burden of kidney disease.
Keywords: Diabetic nephropathy; Glomerular function; Kidney ultrafiltration; Mesenchymal stem cells; Podocyte damage.
Conflict of interest statement
The authors have declared that no conflict of interest.There are no animal experiments carried out for this article.
Figures
References
-
- Sarje SK, Ghiware NB, Kawade RM, Gunjkar VN, Vadvalkar SM. Association of chronic complications of type 2 diabetes with the biochemical and physical estimations in subjects attending single visit screening for complications. Int J Res Pharm Chem. 2013;3:842–845.
-
- Ezquer FE, Ezquer ME, Parrau DB, Carpio D, Yanez AJ, Conget PA. Systemic administration of multipotent mesenchymal stromal cells reverts hyperglycemia and prevents nephropathy in type 1 diabetic mice. Biol Blood Marrow Transpl J Am Soc Blood Marrow Transpl. 2008;14:631–640. doi: 10.1016/j.bbmt.2008.01.006. - DOI - PubMed
-
- Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, et al. Preserving renal function in adults with hypertension and diabetes: a consensus approach. National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J kidney Dis Off J Natl Kidney Found. 2000;36:646–661. doi: 10.1053/ajkd.2000.16225. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous