

Transplant waitlisting attenuates the association between hemodialysis access type and mortality
- PMID: 30604152
- PMCID: PMC6483887
- DOI: 10.1007/s40620-018-00572-0
Transplant waitlisting attenuates the association between hemodialysis access type and mortality
Abstract
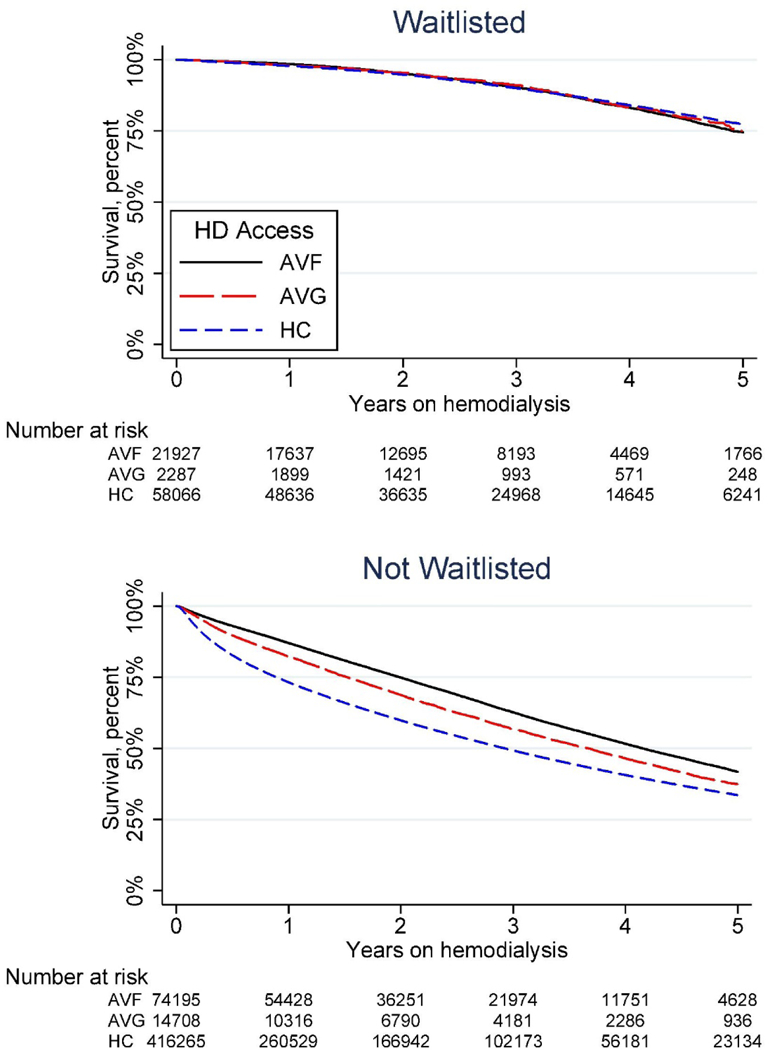
Prior studies have shown that beginning hemodialysis (HD) with a hemodialysis catheter (HC) is associated with worse mortality than with an arteriovenous fistula (AVF) or arteriovenous graft (AVG). We hypothesized that transplant waitlisting would modify the effect of HD access on mortality, given waitlist candidates' more robust health status. Using the US Renal Data System, we studied patients with incident ESRD who initiated HD between 2010 and 2015 with an AVF, AVG, or HC. We used Cox regression including an interaction term for HD access and waitlist status. There were 587,607 patients that initiated HD, of whom 82,379 (14.0%) were waitlisted for transplantation. Only 26,264 (4.5%) were transplanted. Among patients not listed, those with an AVF had a 34% lower mortality compared to HC [adjusted hazard ratio (aHR) 0.66, 95% confidence interval (CI) 0.65-0.67] while those with an AVG had a 21% lower mortality compared to HC (aHR 0.79, 95% CI 0.77-0.81). Transplant waitlisting attenuated the association between hemodialysis access type and mortality (interaction p < 0.001 for both AVF and AVG vs. HC). Among patients on the waitlist, those with an AVF had a 12% lower mortality compared to HC (aHR 0.88, 95% CI 0.84-0.93), while those with an AVG had no difference in mortality (aHR 0.95, 95% CI 0.84-1.08). While all patients benefit from AVF or AVG over HC, the benefit was attenuated in waitlisted patients. Efforts to improve health status and access to healthcare for non-waitlisted ESRD patients might decrease HD-associated mortality and improve rates of AVF and AVG placement.
Keywords: End-stage renal disease; Hemodialysis access; Kidney transplantation; Transplant waitlisting.
Figures

References
-
- Saran R, Robinson B, Abbott KC, Agodoa LYC, Bhave N, Bragg-Gresham J, Balkrishnan R, Dietrich X, Eckard A, Eggers PW, Gaipov A, Gillen D, Gipson D, Hailpern SM, Hall YN, Han Y, He K, Herman W, Heung M, Hirth RA, Hutton D, Jacobsen SJ, Jin Y, Kalantar-Zadeh K, Kapke A, Kovesdy CP, Lavallee D, Leslie J, McCullough K, Modi Z, Molnar MZ, Montez-Rath M, Moradi H, Morgenstern H, Mukhopadhyay P, Nallamothu B, Nguyen DV, Norris KC, O’Hare AM, Obi Y, Park C, Pearson J, Pisoni R, Potukuchi PK, Rao P, Repeck K, Rhee CM, Schrager J, Schaubel DE, Selewski DT, Shaw SF, Shi JM, Shieu M, Sim JJ, Soohoo M, Steffick D, Streja E, Sumida K, Tamura MK, Tilea A, Tong L, Wang D, Wang M, Woodside KJ, Xin X, Yin M, You AS, Zhou H, Shahinian V (2018) US Renal Data System 2017 Annual Data Report: Epidemiology of Kidney Disease in the United States. American journal of kidney diseases : the official journal of the National Kidney Foundation 71 (3s1):A7. doi: 10.1053/j.ajkd.2018.01.002 - DOI - PMC - PubMed
