Medicaid Claims for Contraception Among Women With Medical Conditions After Release of the US Medical Eligibility Criteria for Contraceptive Use
- PMID: 30605421
- PMCID: PMC6341826
- DOI: 10.5888/pcd16.180207
Medicaid Claims for Contraception Among Women With Medical Conditions After Release of the US Medical Eligibility Criteria for Contraceptive Use
Abstract
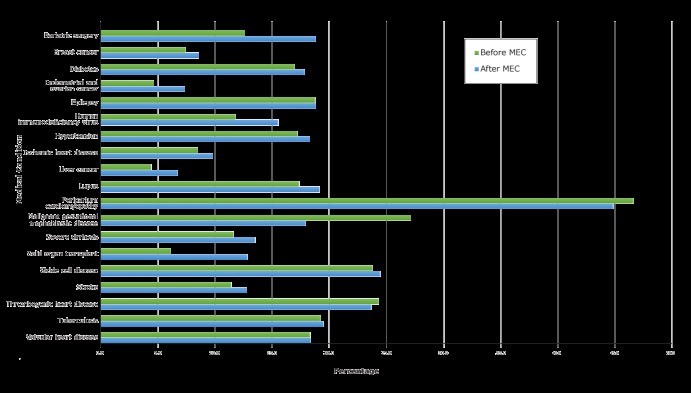
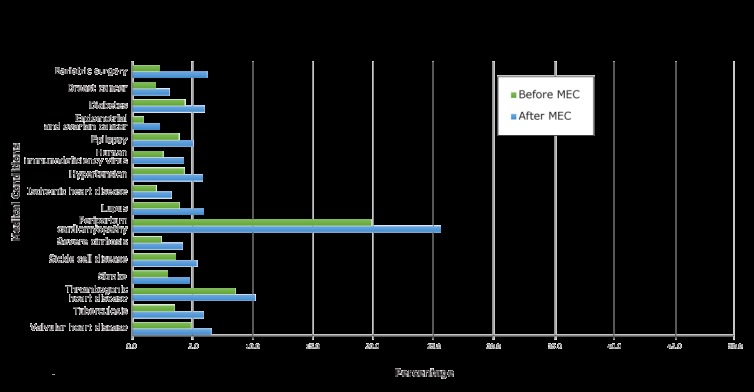
Introduction: The US Medical Eligibility Criteria for Contraceptive Use (MEC) identified 20 medical conditions that increase a woman's risk for adverse outcomes in pregnancy. MEC recommends that women with these conditions use long-acting, highly effective contraceptive methods. The objective of our study was to examine provision of contraception to women enrolled in Medicaid who had 1 or more of these 20 medical conditions METHODS: We used Medicaid Analytic Extract claims data to study Medicaid-enrolled women who were of reproductive age in the 2-year period before MEC's release (2008 and 2009) (N = 442,424) and the 2-year period after its release (2011 and 2012) (N = 533,619) for 14 states. We assessed 2 outcomes: provision of family planning management (FPM) and provision of highest efficacy methods (HEMs) for the entire study population and by health condition. The ratio of the after-MEC rate to the before-MEC rate was used to determine significance in MEC's uptake.
Results: Outcomes increased significantly from the before-MEC period to the after-MEC period for both FPM (1.06; lower bound confidence interval [CI], 1.05) and HEM (1.37; lower bound CI, 1.36) for a 1-sided hypothesis test. For the 19 of 20 conditions we were able to test for FPM, contraceptive use increased significantly for 12 conditions, with ratios ranging from 1.05 to 2.14. For the 16 of 20 conditions tested for HEM, contraception use increased significantly for all conditions, with ratios ranging from 1.19 to 2.80.
Conclusion: Provision of both FPM and HEM increased significantly among women with high-risk health conditions from the before-MEC period (2008 and 2009) to the after-MEC period (2011 and 2012). Health policy makers and clinicians need to continue promotion of effective family planning management for women with high-risk conditions.
Figures
Similar articles
-
Canadian Contraception Consensus (Part 1 of 4).J Obstet Gynaecol Can. 2015 Oct;37(10):936-42. doi: 10.1016/s1701-2163(16)30033-0. J Obstet Gynaecol Can. 2015. PMID: 26606712 English, French.
-
Contraceptive Use and Pregnancy Outcomes Among Women Enrolled in South Carolina Medicaid Programs.Matern Child Health J. 2021 Dec;25(12):1960-1971. doi: 10.1007/s10995-021-03260-x. Epub 2021 Oct 12. Matern Child Health J. 2021. PMID: 34637063
-
Canadian Contraception Consensus (Part 2 of 4).J Obstet Gynaecol Can. 2015 Nov;37(11):1033-9. doi: 10.1016/s1701-2163(16)30054-8. J Obstet Gynaecol Can. 2015. PMID: 26629725 English, French.
-
Evaluation of Medicaid Expansion Under the Affordable Care Act and Contraceptive Care in US Community Health Centers.JAMA Netw Open. 2020 Jun 1;3(6):e206874. doi: 10.1001/jamanetworkopen.2020.6874. JAMA Netw Open. 2020. PMID: 32496568 Free PMC article.
-
Contraceptive use among women with medical conditions: Factors that influence method choice.Semin Perinatol. 2020 Aug;44(5):151310. doi: 10.1016/j.semperi.2020.151310. Epub 2020 Aug 20. Semin Perinatol. 2020. PMID: 32888723 Review.
Cited by
-
Racial Differences in Contraception Encounters and Dispensing Among Female Medicaid Beneficiaries With Systemic Lupus Erythematosus.Arthritis Care Res (Hoboken). 2021 Oct;73(10):1396-1404. doi: 10.1002/acr.24346. Epub 2021 Sep 2. Arthritis Care Res (Hoboken). 2021. PMID: 32526084 Free PMC article.
-
Changes in US health care provider attitudes related to contraceptive safety before and after the release of National Guidance.Contraception. 2019 Nov;100(5):413-419. doi: 10.1016/j.contraception.2019.07.142. Epub 2019 Jul 29. Contraception. 2019. PMID: 31369735 Free PMC article.
-
Contraceptive Use Among Women With End-Stage Kidney Disease on Dialysis in the United States.Kidney Med. 2020 Oct 27;2(6):707-715.e1. doi: 10.1016/j.xkme.2020.08.010. eCollection 2020 Nov-Dec. Kidney Med. 2020. PMID: 33319196 Free PMC article.
-
Association of Pharmacist Prescription With Dispensed Duration of Hormonal Contraception.JAMA Netw Open. 2020 May 1;3(5):e205252. doi: 10.1001/jamanetworkopen.2020.5252. JAMA Netw Open. 2020. PMID: 32432710 Free PMC article.
-
Contraceptive use among women with kidney transplants in the United States.J Nephrol. 2022 Mar;35(2):629-638. doi: 10.1007/s40620-021-01181-0. Epub 2021 Nov 13. J Nephrol. 2022. PMID: 34773601 Free PMC article.
References
-
- Centers for Disease Control and Prevention. US medical eligibility criteria for contraceptive use, 2010. MMWR Morb Mortal Wkly Rep 2010;59(RR–4):1–86. - PubMed
-
- Centers for Disease Control and Prevention. US medical eligibility criteria for contraceptive use, 2016. https://www.cdc.gov/reproductivehealth/contraception/mmwr/mec/summary.html. Accessed March 15, 2018.
-
- Russo JA, Chen BA, Creinin MD. Primary care physician familiarity with U.S. medical eligibility for contraceptive use. Fam Med 2015;47(1):15–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical