

Occurrence of disputed rpoB mutations among Mycobacterium tuberculosis isolates phenotypically susceptible to rifampicin in a country with a low incidence of multidrug-resistant tuberculosis
- PMID: 30606116
- PMCID: PMC6318973
- DOI: 10.1186/s12879-018-3638-z
Occurrence of disputed rpoB mutations among Mycobacterium tuberculosis isolates phenotypically susceptible to rifampicin in a country with a low incidence of multidrug-resistant tuberculosis
Abstract
Background: Accurate drug susceptibility testing (DST) of Mycobacterium tuberculosis in clinical specimens and culture isolates to first-line drugs is crucial for diagnosis and management of multidrug-resistant tuberculosis (MDR-TB). Resistance of M. tuberculosis to rifampicin is mainly due to mutations in hot-spot region of rpoB gene (HSR-rpoB). The prevalence of disputed (generally missed by rapid phenotypic DST methods) rpoB mutations, which mainly include L511P, D516Y, H526N, H526L, H526S, and L533P in HSR-rpoB and I572F in cluster II region of rpoB gene, is largely unknown. This study determined the occurrence of all disputed mutations in HSR-rpoB and at rpoB codon 572 in M. tuberculosis strains phenotypically susceptible to rifampicin in Kuwait.
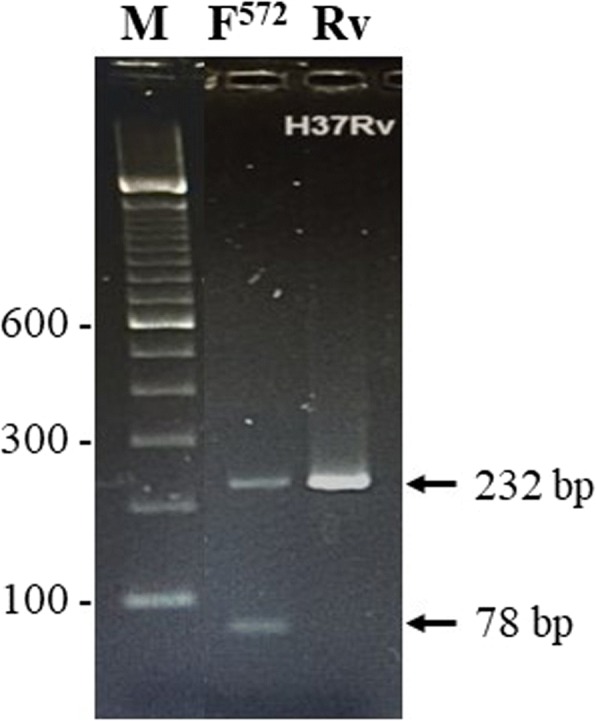
Methods: A total of 242 M. tuberculosis isolates phenotypically susceptible to rifampicin were used. The DST against first-line drugs was performed by Mycobacteria growth indicator tube (MGIT) 960 system. Mutations in HSR-rpoB (and katG codon 315 and inhA-regulatory region for isoniazid resistance) were detected by GenoType MDBDRplus assay. The I572F mutation in cluster II region of rpoB was detected by developing a multiplex allele-specific (MAS)-PCR assay. Results were confirmed by PCR-sequencing of respective loci. Molecular detection of resistance for ethambutol and pyrazinamide and fingerprinting by spoligotyping were also performed for isolates with an rpoB mutation.
Results: Among 242 rifampicin-susceptible isolates, 0 of 130 pansusceptible/monodrug-resistant isolates but 4 of 112 polydrug-resistant isolates contained a disputed rpoB mutation. All 4 isolates were also resistant to isoniazid and molecular screening identified additional resistance to pyrazinamide and ethambutol in one isolate each. In final analysis, 2 of 4 isolates were resistant to all 4 first-line drugs. Spoligotyping showed that the isolates belonged to different M. tuberculosis lineages.
Conclusions: Four of 242 (1.7%) rifampicin-susceptible M. tuberculosis isolates contained a disputed rpoB mutation including 2 isolates resistant to all four first-line drugs. The occurrence of a disputed rpoB mutation in polydrug-resistant M. tuberculosis isolates resistant at least to isoniazid (MDR-TB) suggests that polydrug-resistant strains should be checked for genotypic rifampicin resistance for optimal patient management since the failure/relapse rates are nearly same in isolates with a canonical or disputed rpoB mutation.
Keywords: Mycobacterium tuberculosis; Polydrug resistance; Prevalence; rpoB disputed mutations.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved and the need for written informed consent from patients was waived by the Health Sciences Center Ethics Committee, Faculty of Medicine, Kuwait University (Approval no. VDR/EC/2947 dated 13-12-2016).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organization. Global tuberculosis report . Who/HTM/TB/2017.23. Geneva, Switzerland: WHO; 2017. p. 2017.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
