

Mobility related physical and functional losses due to aging and disease - a motivation for lower limb exoskeletons
- PMID: 30606194
- PMCID: PMC6318939
- DOI: 10.1186/s12984-018-0458-8
Mobility related physical and functional losses due to aging and disease - a motivation for lower limb exoskeletons
Erratum in
-
Correction to: Mobility related physical and functional losses due to aging and disease - a motivation for lower limb exoskeletons.J Neuroeng Rehabil. 2020 Feb 19;17(1):26. doi: 10.1186/s12984-020-0648-z. J Neuroeng Rehabil. 2020. PMID: 32075668 Free PMC article.
Abstract
Background: Physical and functional losses due to aging and diseases decrease human mobility, independence, and quality of life. This study is aimed at summarizing and quantifying these losses in order to motivate solutions to overcome them with a special focus on the possibilities by using lower limb exoskeletons.
Methods: A narrative literature review was performed to determine a broad range of mobility-related physical and functional measures that are affected by aging and selected cardiovascular, respiratory, musculoskeletal, and neurological diseases.
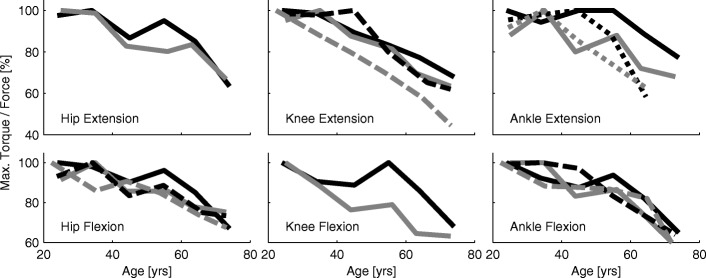
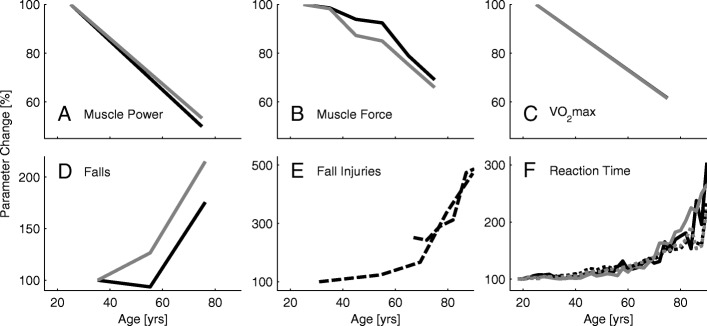
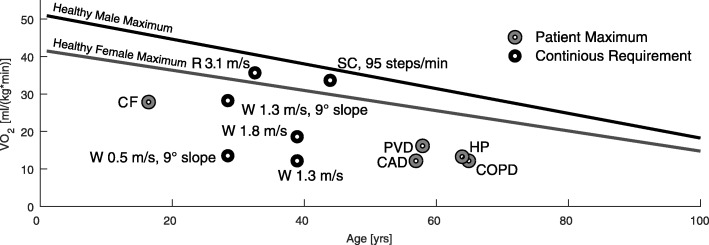
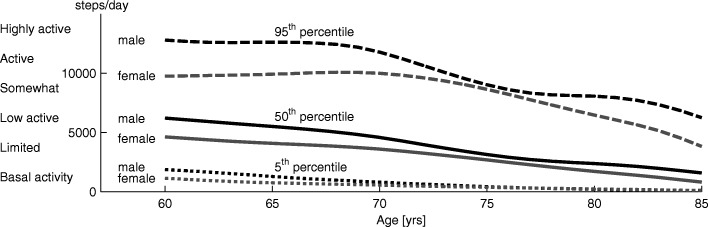
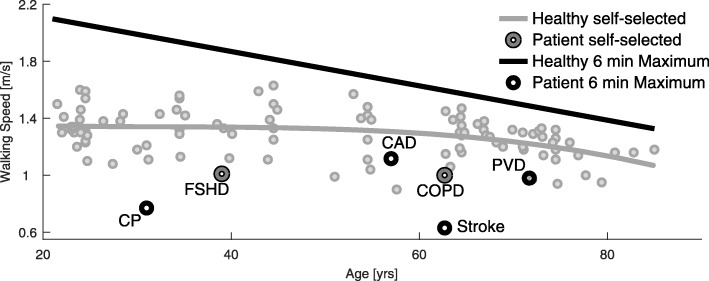
Results: The study identified that decreases in limb maximum muscle force and power (33% and 49%, respectively, 25-75 yrs) and in maximum oxygen consumption (40%, 20-80 yrs) occur for older adults compared to young adults. Reaction times more than double (18-90 yrs) and losses in the visual, vestibular, and somatosensory systems were reported. Additionally, we found decreases in steps per day (75%, 60-85 yrs), maximum walking speed (24% 25-75 yrs), and maximum six-minute and self-selected walking speed (38% and 21%, respectively, 20-85 yrs), while we found increases in the number of falls relative to the number of steps per day (800%), injuries due to falls (472%, 30-90 yrs) and deaths caused by fall (4000%, 65-90 yrs). Measures were identified to be worse for individuals with impaired mobility. Additional detrimental effects identified for them were the loss of upright standing and locomotion, freezing in movement, joint stress, pain, and changes in gait patterns.
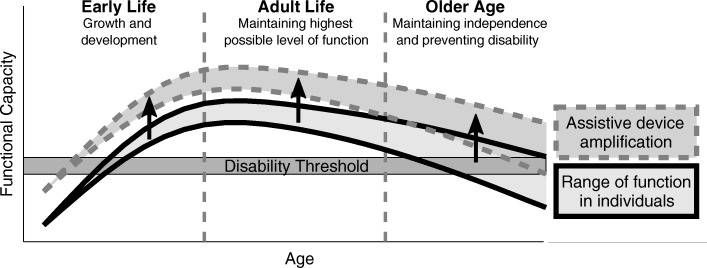
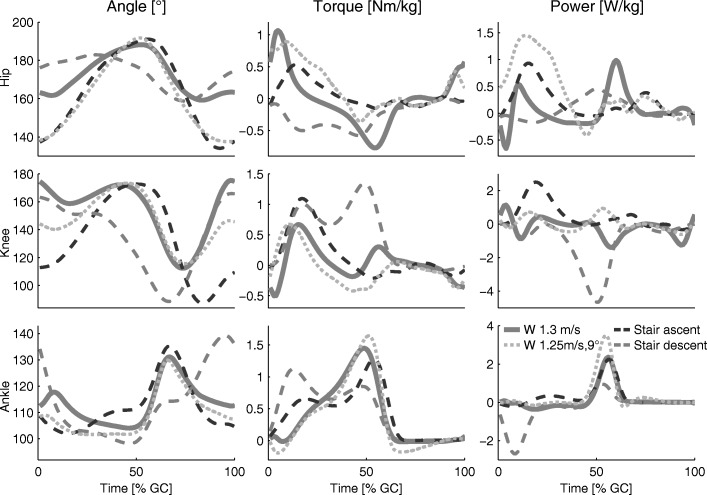
Discussion: This review shows that aging and chronic conditions result in wide-ranging losses in physical and sensory capabilities. While the impact of these losses are relatively modest for level walking, they become limiting during more demanding tasks such as walking on inclined ground, climbing stairs, or walking over longer periods, and especially when coupled with a debilitating disease. As the physical and functional parameters are closely related, we believe that lost functional capabilities can be indirectly improved by training of the physical capabilities. However, assistive devices can supplement the lost functional capabilities directly by compensating for losses with propulsion, weight support, and balance support.
Conclusions: Exoskeletons are a new generation of assistive devices that have the potential to provide both, training capabilities and functional compensation, to enhance human mobility.
Keywords: Aging; Assistance; Exoskeleton; Impaired; Mobility; Motivation; Walking.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors gave their final approval of the submitted version.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
