

Number and cost of hospitalizations with principal and secondary diagnoses of tuberculosis, United States
- PMID: 30606323
- PMCID: PMC8050949
- DOI: 10.5588/ijtld.18.0260
Number and cost of hospitalizations with principal and secondary diagnoses of tuberculosis, United States
Abstract
Objective: To estimate the number and cost of hospitalizations with a diagnosis of active tuberculosis (TB) disease in the United States.
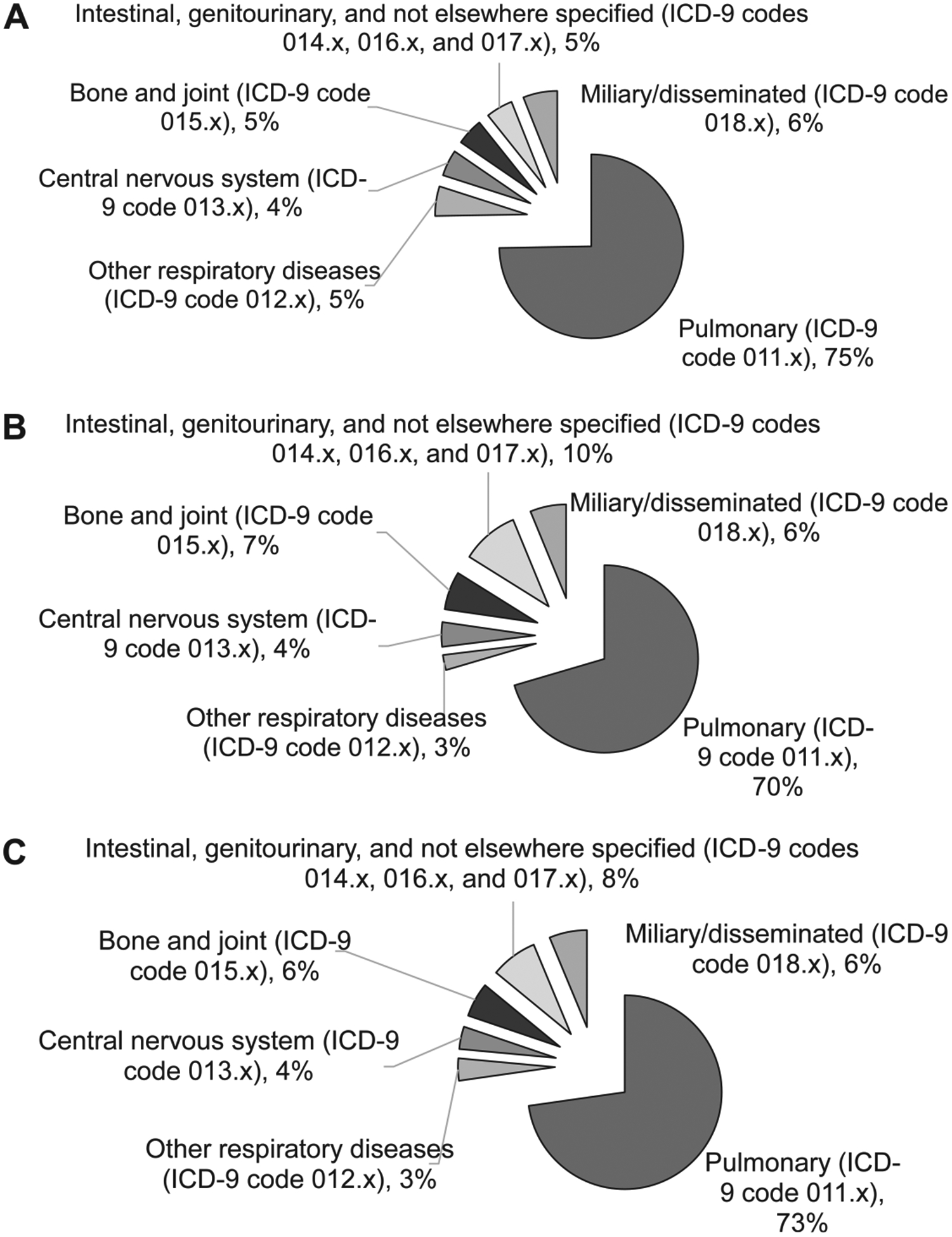
Methods: We analyzed the 2014 National In-Patient Sample using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9) codes to identify hospitalizations with a principal (TB-PD) or any secondary discharge (TB-SD) TB diagnosis. We used a generalized linear model with log link and gamma distribution to estimate the cost per TB-PD and TB-SD episode adjusted for patient demographics, insurer, clinical elements, and hospital characteristics.
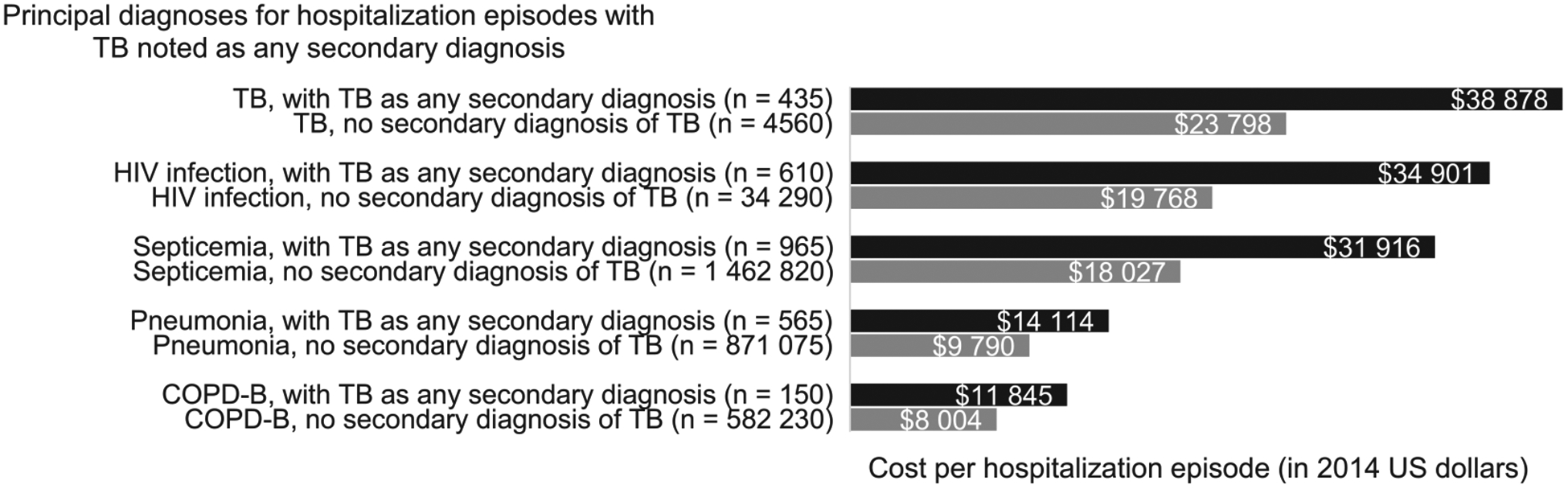
Results: We estimated 4985 TB-PD and 6080 TB-SD hospitalizations nationwide. TB-PD adjusted averaged $16 695 per episode (95%CI $16 168-$17 221). The average for miliary/disseminated TB ($22 498, 95%CI $21 067-$23 929) or TB of the central nervous system ($28 338, 95%CI $25 836-$30 840) was significantly greater than for pulmonary TB ($14 819, 95%CI $14 284-$15 354). The most common principal diagnoses for TB-SD were septicemia (n = 965 hospitalizations), human immunodeficiency virus infection (n = 610), pneumonia (n = 565), and chronic obstructive pulmonary disease and bronchiectasis (COPD-B, n = 150). The adjusted average cost per TB-SD episode was $15 909 (95%CI $15 337-$16 481), varying between $8687 (95%CI $8337-$9036) for COPD-B and $23 335 (95%CI $21 979-$24 690) for septicemia. TB-PD cost the US health care system $123.4 million (95%CI $106.3-$140.5) and TB-SD cost $141.9 million ($128.4-$155.5), of which Medicaid/Medicare covered respectively 67.2% and 69.7%.
Conclusions: TB hospitalizations result in substantial costs within the US health care system.
OBJECTIF :: Estimer le nombre et le coût des hospitalisations liées à un diagnostic de tuberculose (TB) aux Etats-Unis.
MÉTHODE :: Analyser l’échantillon national des patients hospitalisés de 2014 et les codes de l’International Classification of Diseases, Ninth Revision (ICD-9) afin d’identifier les hospitalisations avec une TB comme diagnostic de sortie principal (TB-PD) ou secondaire (TB-SD). Nous avons utilisé un modèle linéaire généralisé avec lien de connexion et distribution gamma pour estimer le coût par épisode de TB-PD et TB-SD, ajusté aux caractéristiques des patients en termes de démographie, d’assurance, d’éléments cliniques et d’hôpital.
RÉSULTATS :: Nous avons estimé 4985 hospitalisations pour TB-PD et 6080 pour TB-SD dans tout le pays. Le coût ajusté de la TB-PD a été en moyenne de $16695 par épisode (IC95% 16168–17221). Le coût moyen d’une TB miliaire/disséminée ($22 498, IC95% 21067–23929) ou d’une TB du systéme nerveux central ($28 338, IC95% 25 836–30 840) a été significativement plus élevé que celui de la TB pulmonaire ($ 14819, IC95% 14284–15354). Les diagnostics principaux les plus fréquents de la TB-SD ont été une septicémie (n = 965 hospitalisations), une infection au virus de l’immunodéficience humaine (n = 610), une pneumonie (n = 565), et une broncho-pneumopathie chronique obstructive et une bronchectasie (BPCO-B; n = 150 hospitalisations). Le coût ajusté moyen par épisode de TB-SD a été de $15909 (IC95% 15337–16481), variant de $8687 (IC95% 8337–9036) pour les BPCO-B à $23335 (IC95% 21 979–24690) pour une septicémie. Le coût de la TB-PD dans le système de santé des Etats-Unis atteint 123,4 millions (IC95% 106,3–140,5) de dollars et celui de la TB-SD, 141,9 millions (IC95% 128,4–155,5) de dollars, dont Medicaid et Medicare a couvert 67,2% et 69,7%, respectivement.
CONCLUSION :: Les hospitalisations pour TB ont un coût substantiel en termes de services de santé au sein du système de soins de santé américain.
OBJETIVO:: Estimar el número de hospitalizaciones con un diagnóstico de tuberculosis (TB) activa y su costo en los Estados Unidos.
MÉTODOS:: Se analizó una muestra nacional de pacientes hospitalizados en el 2014, utilizando los códigos de la International Classification of Diseases, Ninth Revision (ICD-9) con el fin de reconocer las hospitalizaciones donde el diagnóstico principal de alta fue TB activa (TB-PD) y aquellas con TB activa como alguno de los diagnósticos secundarios de alta (TB-SD). Se aplicó un modelo lineal generalizado con función de enlace logarítmica y distribución con el objeto de estimar el costo por episodio de TB-PD y de TB-SD ajustado con respecto a las características demográficas, la aseguradora y las características clínicas del paciente y las características del hospital.
RESULTADOS:: Se calcularon 4985 hospitalizaciones con TB-PD y 6080 con TB-SD en todo el país. El promedio ajustado por episodio de TB-PD fue 16695 dólares (IC95% 16168–17221). El costo promedio por episodio de TB miliar o diseminada (22498 dólares; IC95% 21067–23929) o por TB del sistema nervioso central (28338 dólares; IC95% 25836–30840) fue significativamente mayor que por episodio de TB pulmonar (14819 dólares; IC95% 14284–15354). Los diagnósticos principales más frecuentes en los casos de TB-SD fueron septicemia (n = 965 hospitalizaciones), infección por el virus de la inmunodeficiencia humana (n = 610), neumonía (n = 565), enfermedad pulmonar obstructiva crónica y bronquiectasias (EPOC-B; n = 150 hospitalizaciones). El costo promedio ajustado por episodio de TB-SD fue 15909 dólares (IC95% 15337–16481) y osciló entre 8687 dólares (IC95% 8337–9036) en caso de EPOC-B y 23335 dólares (IC95% 21979–24690) en caso de septicemia. En el 2014, los casos de TB-PD costaron al sistema de salud de los Estados Unidos 123,4 millones de dólares (IC95% 106,3–140,5 millones) y los de TB-SD costaron 141,9 millones de dólares (IC95% 128,4–155,5 millones), de los cuales Medicaid cubrió el 67,2% y Medicare el 69,7%.
CONCLUSIÓN:: Las hospitalizaciones por TB originan costos considerables al sistema de salud de los Estados Unidos.
Conflict of interest statement
Conflicts of interest: none declared.
Figures
Similar articles
-
Tuberculosis hospitalization expenditures per patient from private health insurance claims data, 2010-2014.Int J Tuberc Lung Dis. 2017 Apr 1;21(4):398-404. doi: 10.5588/ijtld.16.0587. Int J Tuberc Lung Dis. 2017. PMID: 28284254 Free PMC article.
-
Causes and costs of hospitalization of tuberculosis patients in the United States.Int J Tuberc Lung Dis. 2000 Oct;4(10):931-9. Int J Tuberc Lung Dis. 2000. PMID: 11055760 Free PMC article.
-
Pulmonary vs. extra-pulmonary tuberculosis hospitalizations in the US [1998-2014].J Infect Public Health. 2020 Jan;13(1):131-139. doi: 10.1016/j.jiph.2019.07.001. Epub 2019 Aug 14. J Infect Public Health. 2020. PMID: 31422038
-
Effect of HIV infection and tuberculosis on hospitalizations and cost of care for young adults in the United States, 1985 to 1990.Ann Intern Med. 1994 Nov 15;121(10):786-92. doi: 10.7326/0003-4819-121-10-199411150-00009. Ann Intern Med. 1994. PMID: 7944056
-
[Hospitalization of tuberculosis patients in Swiss hospitals in 1990].Schweiz Med Wochenschr. 1992 Dec 5;122(49):1875-82. Schweiz Med Wochenschr. 1992. PMID: 1462148 German.
Cited by
-
Burden of Active Tuberculosis in an Integrated Health Care System, 1997-2016: Incidence, Mortality, and Excess Health Care Utilization.Open Forum Infect Dis. 2020 Jan 12;7(1):ofaa015. doi: 10.1093/ofid/ofaa015. eCollection 2020 Jan. Open Forum Infect Dis. 2020. PMID: 32010737 Free PMC article.
-
Epidemiology and Prevention of Tuberculosis and Chronic Hepatitis B Virus Infection in the United States.J Immigr Minor Health. 2021 Dec;23(6):1267-1279. doi: 10.1007/s10903-021-01231-6. Epub 2021 Jun 23. J Immigr Minor Health. 2021. PMID: 34160726 Review.
-
Cost-effectiveness of expanded latent TB infection testing and treatment: Lynn City, Massachusetts, USA.Int J Tuberc Lung Dis. 2024 Jan 1;28(1):21-28. doi: 10.5588/ijtld.22.0654. Int J Tuberc Lung Dis. 2024. PMID: 38178297 Free PMC article.
-
Estimated Costs of 4-Month Pulmonary Tuberculosis Treatment Regimen, United States.Emerg Infect Dis. 2023 Oct;29(10):2102-2104. doi: 10.3201/eid2910.230314. Emerg Infect Dis. 2023. PMID: 37735769 Free PMC article.
-
Cost-effectiveness of video-observed therapy for ambulatory management of active tuberculosis during the COVID-19 pandemic in a high-income country.Int J Infect Dis. 2021 Dec;113:271-278. doi: 10.1016/j.ijid.2021.10.029. Epub 2021 Oct 22. Int J Infect Dis. 2021. PMID: 34688946 Free PMC article.
References
-
- American Thoracic Society, Centers for Disease Control and Prevention, Infectious Diseases Society of America. Treatment of tuberculosis. MMWR Recomm Rep 2003; 52(RR-11): 1–77. - PubMed
-
- Centers for Disease Control and Prevention. Reported tuberculosis in the United States, 2014. Atlanta, GA, USA: US Department of Health and Human Services, CDC, 2015. https://www.cdc.gov/tb/statistics/reports/2014/default.htm. Accessed September 2018.
-
- Brown RE, Miller B, Taylor WR, et al. Health-care expenditures for tuberculosis in the United States. Arch Intern Med 1995; 155: 1595–1600. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
