

Relation between Chlamydia trachomatis infection and pelvic inflammatory disease, ectopic pregnancy and tubal factor infertility in a Dutch cohort of women previously tested for chlamydia in a chlamydia screening trial
- PMID: 30606817
- PMCID: PMC6585279
- DOI: 10.1136/sextrans-2018-053778
Relation between Chlamydia trachomatis infection and pelvic inflammatory disease, ectopic pregnancy and tubal factor infertility in a Dutch cohort of women previously tested for chlamydia in a chlamydia screening trial
Abstract
Objectives: A better understanding of Chlamydia trachomatis infection (chlamydia)-related sequelae can provide a framework for effective chlamydia control strategies. The objective of this study was to estimate risks and risk factors of pelvic inflammatory disease (PID), ectopic pregnancy and tubal factor infertility (TFI) with a follow-up time of up until 8 years in women previously tested for chlamydia in the Chlamydia Screening Implementation study (CSI) and participating in the Netherlands Chlamydia Cohort Study (NECCST).
Methods: Women who participated in the CSI 2008-2011 (n=13 498) were invited in 2015-2016 for NECCST. Chlamydia positive was defined as a positive CSI-PCR test, positive chlamydia serology and/or self-reported infection (time dependent). Data on PID, ectopic pregnancy and TFI were collected by self-completed questionnaires. Incidence rates and HRs were compared between chlamydia-positive and chlamydia-negative women corrected for confounders.
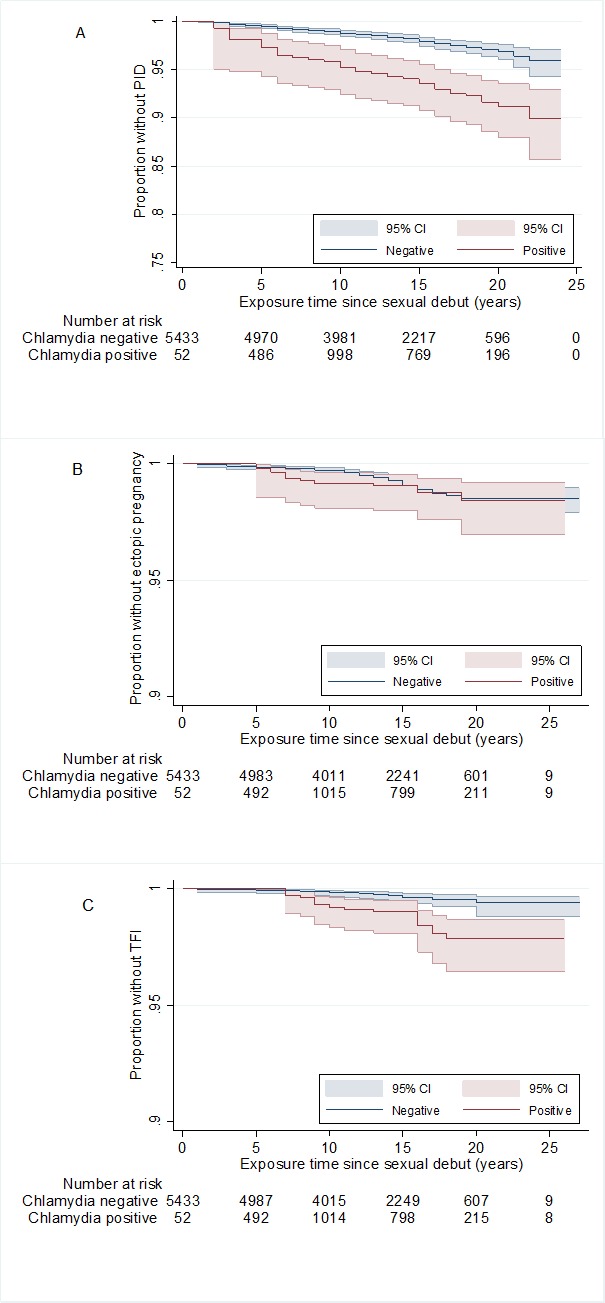
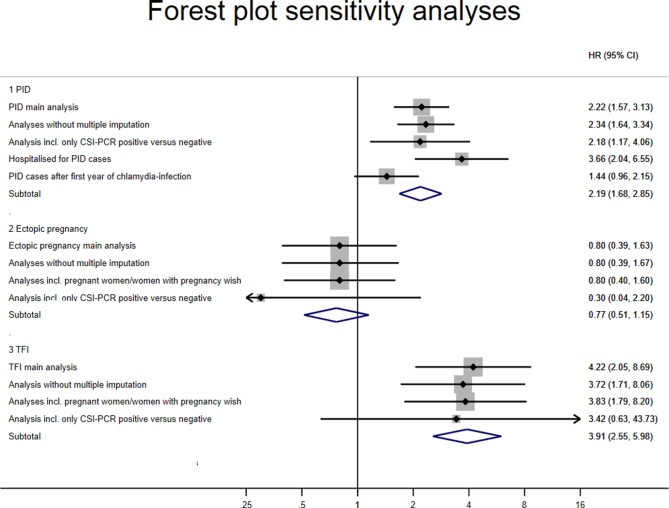
Results: Of 5704 women included, 29.5% (95% CI 28.3 to 30.7) were chlamydia positive. The incidence rate of PID was 1.8 per 1000 person-years (py) (1.6 to 2.2) overall, 4.4 per 1000 py (3.3 to 5.7) among chlamydia positives compared with 1.4 per 1000 py (1.1 to 1.7) for chlamydia negatives. For TFI, this was 0.4 per 1000 py (0.3 to 0.5) overall, 1.3 per 1000 py (0.8 to 2.1) and 0.2 per 1000 py (0.1 to 0.4) among chlamydia positives and negatives, respectively. And for ectopic pregnancy, this was 0.6 per 1000 py (0.5 to 0.8) overall, 0.8 per 1000 py (0.4 to 1.5) and 0.6 per 1000 py (0.4 to 0.8) for chlamydia negatives. Among chlamydia-positive women, the strongest risk factor for PID was symptomatic versus asymptomatic infection (adjusted HR 2.88, 1.4 to 4.5) and for TFI age <20 versus >24 years at first infection (HR 4.35, 1.1 to 16.8).
Conclusion: We found a considerably higher risk for PID and TFI in chlamydia-positive women, but the incidence for ectopic pregnancy was comparable between chlamydia-positive and chlamydia-negative women. Overall, the incidence rates of sequelae remained low.
Trial registration: NTR-5597.
Keywords: chlamydia trachomatis; cohort study; ectopic pregnancy; pelvic inflammatory disease; serology; tubal factor infertility.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
The Netherlands Chlamydia cohort study (NECCST) protocol to assess the risk of late complications following Chlamydia trachomatis infection in women.BMC Infect Dis. 2017 Apr 11;17(1):264. doi: 10.1186/s12879-017-2376-y. BMC Infect Dis. 2017. PMID: 28399813 Free PMC article.
-
The natural history of Chlamydia trachomatis infection in women: a multi-parameter evidence synthesis.Health Technol Assess. 2016 Mar;20(22):1-250. doi: 10.3310/hta20220. Health Technol Assess. 2016. PMID: 27007215 Free PMC article. Review.
-
Chlamydia infection, pelvic inflammatory disease, ectopic pregnancy and infertility: cross-national study.Sex Transm Infect. 2011 Dec;87(7):601-8. doi: 10.1136/sextrans-2011-050205. Epub 2011 Oct 25. Sex Transm Infect. 2011. PMID: 22028428
-
Chlamydia trachomatis: impact on human reproduction.Hum Reprod Update. 1999 Sep-Oct;5(5):433-47. doi: 10.1093/humupd/5.5.433. Hum Reprod Update. 1999. PMID: 10582782 Review.
-
Diagnosed Gonorrhea Among Privately Insured Women: Analysis of United States Claims Data.J Womens Health (Larchmt). 2023 Sep;32(9):942-949. doi: 10.1089/jwh.2023.0006. Epub 2023 Jun 29. J Womens Health (Larchmt). 2023. PMID: 37384920 Free PMC article.
Cited by
-
Sequential-contingent strategy for fallopian tube evaluation using hysterosalpingo foam sonography: a cost analysis.Quant Imaging Med Surg. 2024 Jan 3;14(1):540-547. doi: 10.21037/qims-23-816. Epub 2024 Jan 2. Quant Imaging Med Surg. 2024. PMID: 38223069 Free PMC article.
-
Contraceptive effects on the cervicovaginal microbiome: Recent evidence including randomized trials.Am J Reprod Immunol. 2023 Nov;90(5):e13785. doi: 10.1111/aji.13785. Am J Reprod Immunol. 2023. PMID: 37881121 Free PMC article. Review.
-
Brazilian Protocol for Sexually Transmitted infections, 2020: pelvic inflammatory disease.Rev Soc Bras Med Trop. 2021 May 17;54(suppl 1):e2020602. doi: 10.1590/0037-8682-602-2020. eCollection 2021. Rev Soc Bras Med Trop. 2021. PMID: 34008722 Free PMC article.
-
A Large Study About Reproductive Factors That Predict Hysterosalpingography-Identified Tubal Pathology: An Insight into the Necessity of Preconception Screening.J Clin Med. 2024 Dec 31;14(1):179. doi: 10.3390/jcm14010179. J Clin Med. 2024. PMID: 39797266 Free PMC article.
-
Active screening significantly improves detection of chlamydia in women's health clinics in Shaoxing, China.PLoS One. 2025 May 7;20(5):e0321492. doi: 10.1371/journal.pone.0321492. eCollection 2025. PLoS One. 2025. PMID: 40333999 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical