

doi: 10.4081/oncol.2018.397.
eCollection 2018 Jul 4.
Myelodysplastic syndrome from theoretical review to clinical application view
Affiliations
- PMID: 30607219
- PMCID: PMC6291758
- DOI: 10.4081/oncol.2018.397
Item in Clipboard
Myelodysplastic syndrome from theoretical review to clinical application view
Oncol Rev.
.
Abstract
Myelodysplastic syndromes (MDS), called ineffective hematopoiesis is indicated by bone marrow failure and tendency to acute myeloid leukemia transformation. Since the disease is more common in elderly with non- hematology co-morbidities, the research for less toxic and curative novel agents is essential. More than 12 years without new Food and Drug Administration approved drugs in MDS management through the whole course, only 5 drugs. We summarized the basic data in diagnosis, treatment guidelines and future direction.
Keywords: Myelodysplastic syndrome; hypomethyating agents; lenalidomide.
Conflict of interest statement
Conflict of interest: the author declares no conflict of interest.
Figures
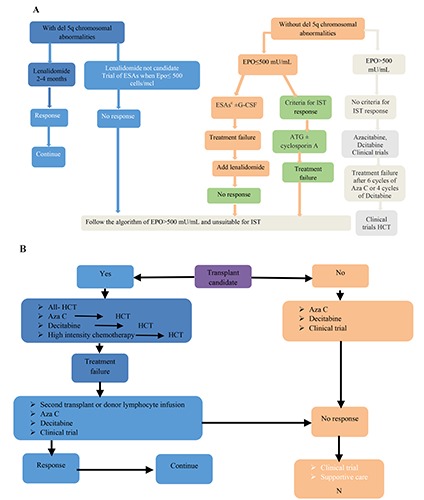
A) Proposed algorithm for low risk (IPSS low, intermediate; IPSS-R or WPSS, very low, low or intermediate) management. Chromosomal abnormality and with symptomatic anemia follow the same algorithm (except chromosome 7). a) The lenalidomide standard dose is 10 mg/day for 3 weeks and 1 week of (3/4), however, in the presence of significant neutropenia (platelet count <25000 cell/mcl) ± neutrophil count <500 cell/mcl), the dose may be modified or withdrawal; b) ESAs included darbepoetin alfa (150-300 mcg SC every other week) and human recombinant Epo (40,000 to 60,000 SC units twice/week); c) Ring sideroblasts .15% in BM and EPO.500 mU/Ml are predictive markers for better response. 1-2mcg/kg twice/week in the standard dose of G-CSF; d) Treatment failure is defined as loss of the response after 3 months. We must exclude iron deficiency. Response evaluation according to IWG; e) Criteria for IST are HLA-DR15 histocompatibility type, low risk, normal cytogenetics, hypocellular BM, and PNH clone. B) Proposed algorithm for high risk MDS (IPSS int-2, high; IPSS-R intermediate, high, very high; WPSS high, very high) management. IST: immunosuppressive treatment, HCT: Hematopoietic stem cell transplantation.
Similar articles
-
Physician Education: Myelodysplastic Syndrome.Oncologist. 1996;1(4):284-287. Oncologist. 1996. PMID: 10388004
-
Novel combinations to improve hematopoiesis in myelodysplastic syndrome.Stem Cell Res Ther. 2020 Mar 20;11(1):132. doi: 10.1186/s13287-020-01647-1. Stem Cell Res Ther. 2020. PMID: 32197634 Free PMC article. Review.
-
Myelodysplastic Syndrome with Transfusion Dependence Treated with Venetoclax.Case Rep Hematol. 2020 Mar 12;2020:9031067. doi: 10.1155/2020/9031067. eCollection 2020. Case Rep Hematol. 2020. PMID: 32231817 Free PMC article.
-
Childhood myelodysplastic syndrome.Indian J Pediatr. 2013 Sep;80(9):764-71. doi: 10.1007/s12098-013-1130-8. Epub 2013 Aug 3. Indian J Pediatr. 2013. PMID: 23912822 Review.
-
[Updated treatment strategies for myelodysplastic syndromes].Rinsho Ketsueki. 2022;63(6):660-666. doi: 10.11406/rinketsu.63.660. Rinsho Ketsueki. 2022. PMID: 36184521 Japanese.
Cited by
-
Canonical Wnt: a safeguard and threat for erythropoiesis.Blood Adv. 2021 Sep 28;5(18):3726-3735. doi: 10.1182/bloodadvances.2021004845. Blood Adv. 2021. PMID: 34516644 Free PMC article. Review.
-
Size-tuneable and immunocompatible polymer nanocarriers for drug delivery in pancreatic cancer.Nanoscale. 2022 May 5;14(17):6656-6669. doi: 10.1039/d2nr00864e. Nanoscale. 2022. PMID: 35438701 Free PMC article.
-
Prognostic Markers of Myelodysplastic Syndromes.Medicina (Kaunas). 2020 Jul 27;56(8):376. doi: 10.3390/medicina56080376. Medicina (Kaunas). 2020. PMID: 32727068 Free PMC article. Review.
-
Comparative study of IgG binding to megakaryocytes in immune and myelodysplastic thrombocytopenic patients.Ann Hematol. 2021 Jul;100(7):1701-1709. doi: 10.1007/s00277-021-04556-2. Epub 2021 May 13. Ann Hematol. 2021. PMID: 33982136
-
Diamond-Blackfan anemia with mutation in RPS19: A case report and an overview of published pieces of literature.J Pharm Bioallied Sci. 2020 Apr-Jun;12(2):163-170. doi: 10.4103/jpbs.JPBS_234_19. Epub 2020 Apr 10. J Pharm Bioallied Sci. 2020. PMID: 32742115 Free PMC article.
References
-
- Steensma DP. Myelodysplastic syndromes: diagnosis and treatment. Mayo Clin Proc 2015;90:969-83. - PubMed
-
- National cancer Institute SEER cancer statistics review, 1975-2013: Myelodysplastic Syndromes (MDS), Chronic Myeloproliferative Disorders (CMD), and Chronic Myelomonocytic Leukemia (CMML). 2016. Available from: https://seer.cancer.gov/archive/csr/1975_2013/browse_csr.php?sectionSEL=...
-
- Goldberg H, Lusk E, Moore J, et al. Survey of exposure to genotoxic agents in primary myelodysplastic syndrome: correlation with chromosome patterns and data on patients without hematological disease. Cancer Res 1990;50:6876-81. - PubMed
-
- Nolte F, Hofmann WK. Molecular mechanisms involved in the progression of myelodysplastic syndrome. Future Oncol 2010;6:445-55. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous