

Impaired right ventricular ejection fraction after cardiac surgery is associated with a complicated ICU stay
- PMID: 30607248
- PMCID: PMC6307315
- DOI: 10.1186/s40560-018-0351-3
Impaired right ventricular ejection fraction after cardiac surgery is associated with a complicated ICU stay
Abstract
Background: Right ventricular (RV) dysfunction is a known risk factor for increased mortality in cardiac surgery. However, the association between RV performance and ICU morbidity is largely unknown.
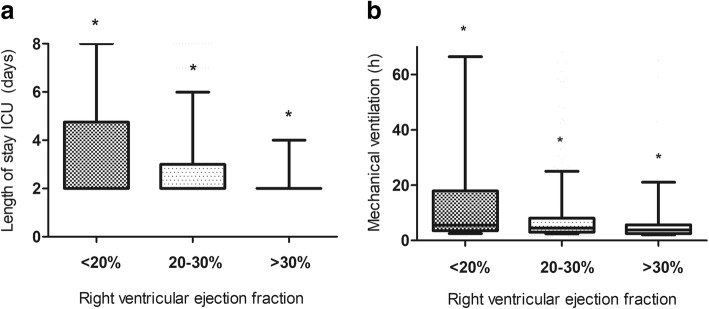
Methods: We performed a single-centre, retrospective study including cardiac surgery patients equipped with a pulmonary artery catheter, enabling continuous right ventricular ejection fraction (RVEF) measurements. Primary endpoint of our study was ICU morbidity (as determined by ICU length of stay, duration of mechanical ventilation, usage of inotropic drugs and fluids, and kidney dysfunction) in relation to RVEF. Patients were divided into three groups according to their RVEF; < 20%, 20-30%, and > 30%.
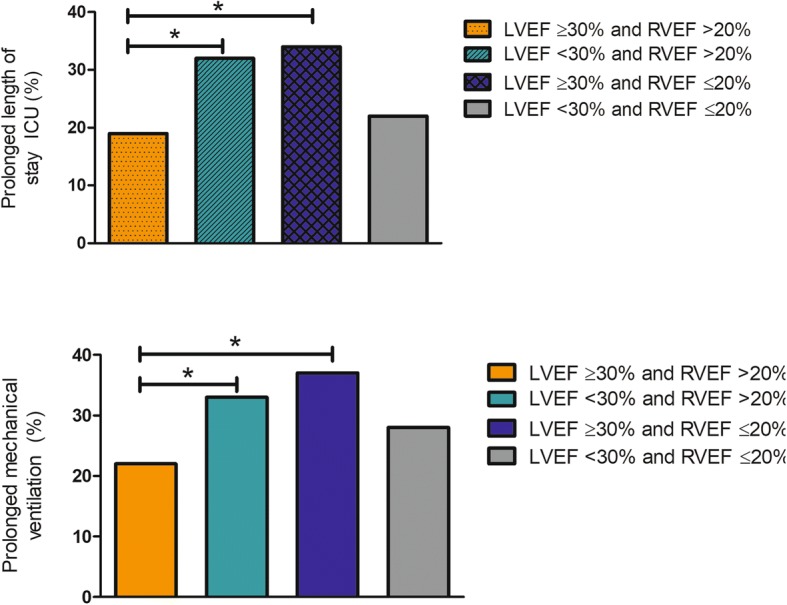
Results: We included 1109 patients. Patients with a RVEF < 20% had a significantly longer stay in ICU, a longer duration of mechanical ventilation, higher fluid balance, a higher incidence of inotropic drug usage, and more increase in postoperative creatinine levels in comparison to the other subgroups. In a multivariate analysis, RVEF was independently associated with increased ICU length of stay (OR 0.934 CI 0.908-0.961, p < 0.001), prolonged duration of mechanical ventilation (OR 0.969, CI 0.942-0.998, p = 0.033), usage of inotropic drugs (OR 0.944, CI 0.917-0.971, p < 0.001), and increase in creatinine (OR 0.962, CI 0.934-0.991, p = 0.011).
Conclusions: A decreased RVEF is independently associated with a complicated ICU stay.
Keywords: Cardiac surgery; Intensive care; Morbidity; Pulmonary artery catheter; Right ventricle; Right ventricular function; Thermodilution.
Conflict of interest statement
The study was approved by the local ethical and scientific committee (“regionale toetsingscommissie patiëntgebonden onderzoek”, registration number nWMO95), and the need for informed consent was waived in accordance with applicable laws.Non applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Identifying risk factors for perioperative decline in right ventricular performance in cardiac surgery patients: a prospective observational study in a tertiary care hospital.BMJ Open. 2023 Feb 24;13(2):e068598. doi: 10.1136/bmjopen-2022-068598. BMJ Open. 2023. PMID: 36828663 Free PMC article.
-
Right Ventricular Function After Cardiac Surgery Is a Strong Independent Predictor for Long-Term Mortality.J Cardiothorac Vasc Anesth. 2017 Oct;31(5):1656-1662. doi: 10.1053/j.jvca.2017.02.008. Epub 2017 Feb 5. J Cardiothorac Vasc Anesth. 2017. PMID: 28416392
-
Right Ventricular Function and Long-Term Outcome in Sepsis: A Retrospective Cohort Study.Shock. 2020 May;53(5):537-543. doi: 10.1097/SHK.0000000000001413. Shock. 2020. PMID: 31318835
-
[High preoperative pulmonary artery systolic pressure is associated with acute kidney injury and prognosis in patients underwent cardiopulmonary bypass surgery].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Mar;32(3):319-323. doi: 10.3760/cma.j.cn121430-20200224-00073. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32385996 Chinese.
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
Cited by
-
Right ventricular ejection fraction derived from intraoperative three-dimensional transesophageal echocardiography versus cardiac magnetic resonance imaging.Can J Anaesth. 2023 Oct;70(10):1576-1586. doi: 10.1007/s12630-023-02569-1. Epub 2023 Sep 26. Can J Anaesth. 2023. PMID: 37752378 English.
-
Impact of the right ventricular mechanical pattern assessed by three-dimensional echocardiography on adverse outcomes following cardiac surgery.Sci Rep. 2025 Feb 15;15(1):5623. doi: 10.1038/s41598-025-89122-w. Sci Rep. 2025. PMID: 39955387 Free PMC article.
-
Effect of Preoperative Pulmonary Hypertension on the Course of Right Ventricular Function: A Three-dimensional Echocardiographic Study in Valvular Surgery Patients.J Cardiovasc Echogr. 2024 Oct-Dec;34(4):170-178. doi: 10.4103/jcecho.jcecho_38_24. Epub 2024 Dec 19. J Cardiovasc Echogr. 2024. PMID: 39895890 Free PMC article.
-
Predictors of Outcome in Patients with Pulmonary Hypertension Undergoing Mitral and Tricuspid Valve Surgery.Medicina (Kaunas). 2023 Jun 7;59(6):1103. doi: 10.3390/medicina59061103. Medicina (Kaunas). 2023. PMID: 37374307 Free PMC article.
-
The Outcomes of Coronary Artery Bypass Surgery after 18 Months-Is There an Influence of the Initial Right Ventricle Diastolic Dysfunction?J Cardiovasc Dev Dis. 2023 Jan 4;10(1):18. doi: 10.3390/jcdd10010018. J Cardiovasc Dev Dis. 2023. PMID: 36661913 Free PMC article.
References
-
- Parsonnet V, Dean D, Bernstein AD. A method of uniform stratification of risk for evaluating the results of surgery in acquired adult heart disease. Circulation. 1989;79(6 Pt 2):I3–12. - PubMed
LinkOut - more resources
Full Text Sources
