

Experience in Rehabilitation Medicine Affects Prognosis and End-of-Life Decision-Making of Neurologists: A Case-Based Survey
- PMID: 30607828
- PMCID: PMC6611059
- DOI: 10.1007/s12028-018-0661-2
Experience in Rehabilitation Medicine Affects Prognosis and End-of-Life Decision-Making of Neurologists: A Case-Based Survey
Abstract
Background: Outcome predictions in patients with acute severe neurologic disorders are difficult and influenced by multiple factors. Since the decision for and the extent of life-sustaining therapies are based on the estimated prognosis, it is vital to understand which factors influence such estimates. This study examined whether previous professional experience with rehabilitation medicine influences physician decision-making.
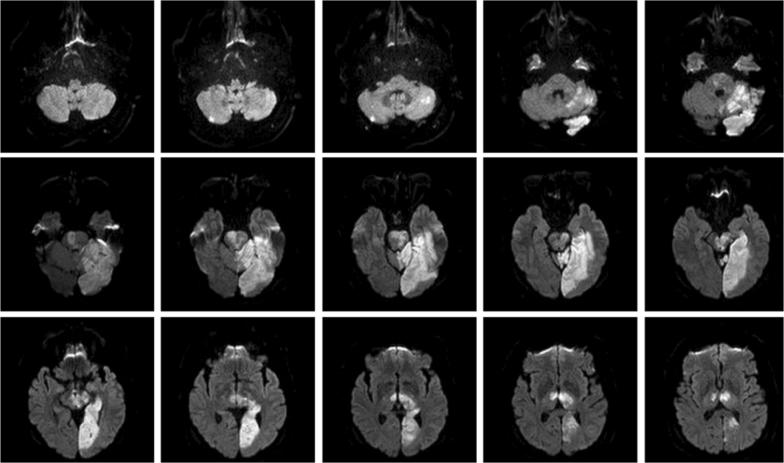
Methods: A case vignette presenting a typical patient with an extensive brain stem infarction was developed and distributed online to clinical neurologists. Questions focused on prognosis, interpretation of an advanced directive, whether to withdraw life-sustaining treatments and information on prior rehabilitation experience from the survey respondent.
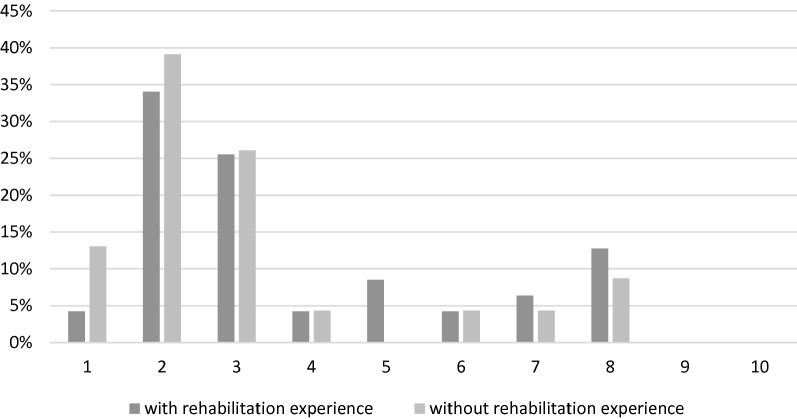
Results: Of the participating neurologists, 77% opted for the withdrawal of life-sustaining therapies (n = 70; response rate: 14.8%). This decision was not affected by age, gender, or length of clinical experience. Neurologists with experience in rehabilitation medicine tended to estimate a more positive prognosis than neurologists without, but this result was not significant (p = .13). There was an association between the intervention chosen and previous experience in rehabilitation; neurologists with experience in rehabilitation medicine opted significantly more often (31.8%) for continuing life-sustaining treatments than neurologists without such experience (8.7%, p = .04).
Conclusion: Our results indicate that there are subjective factors influencing decisions to limit life-sustaining treatments that are based on previous professional experience. This finding emphasizes the variability and cognitive bias of such decision processes and should be integrated into future guidelines for specialist training on end-of-life decision-making.
Keywords: Disorder of consciousness; End-of-life decision; Life-sustaining therapy; Neurointensive care; Prognosis; Stroke.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Mayer SA, Kossoff SB. Withdrawal of life support in the neurological intensive care unit. Neurology. 1999;52(8):1602–1609. - PubMed
-
- Forte D, Vincent JL, Velasco IT, Park M. Association between education in EOL care and variability in EOL practice: a survey of ICU physicians. Intensive Care Med. 2012;38(1):404–412. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
