

Incidence, Risk Factors, and Outcomes of Intra-Abdominal Hypertension in Critically Ill Patients-A Prospective Multicenter Study (IROI Study)
- PMID: 30608280
- PMCID: PMC6426342
- DOI: 10.1097/CCM.0000000000003623
Incidence, Risk Factors, and Outcomes of Intra-Abdominal Hypertension in Critically Ill Patients-A Prospective Multicenter Study (IROI Study)
Abstract
Objectives: To identify the prevalence, risk factors, and outcomes of intra-abdominal hypertension in a mixed multicenter ICU population.
Design: Prospective observational study.
Setting: Fifteen ICUs worldwide.
Patients: Consecutive adult ICU patients with a bladder catheter.
Interventions: None.
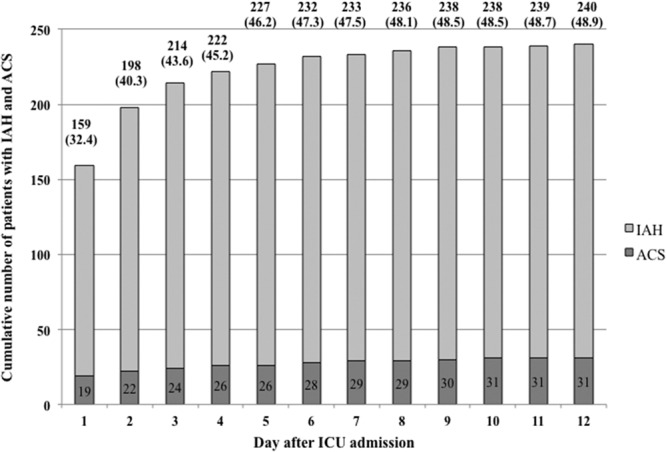
Measurements and main results: Four hundred ninety-one patients were included. Intra-abdominal pressure was measured a minimum of every 8 hours. Subjects with a mean intra-abdominal pressure equal to or greater than 12 mm Hg were defined as having intra-abdominal hypertension. Intra-abdominal hypertension was present in 34.0% of the patients on the day of ICU admission (159/467) and in 48.9% of the patients (240/491) during the observation period. The severity of intra-abdominal hypertension was as follows: grade I, 47.5%; grade II, 36.6%; grade III, 11.7%; and grade IV, 4.2%. The severity of intra-abdominal hypertension during the first 2 weeks of the ICU stay was identified as an independent predictor of 28- and 90-day mortality, whereas the presence of intra-abdominal hypertension on the day of ICU admission did not predict mortality. Body mass index, Acute Physiology and Chronic Health Evaluation II score greater than or equal to 18, presence of abdominal distension, absence of bowel sounds, and positive end-expiratory pressure greater than or equal to 7 cm H2O were independently associated with the development of intra-abdominal hypertension at any time during the observation period. In subjects without intra-abdominal hypertension on day 1, body mass index combined with daily positive fluid balance and positive end-expiratory pressure greater than or equal to 7 cm H2O (as documented on the day before intra-abdominal hypertension occurred) were associated with the development of intra-abdominal hypertension during the first week in the ICU.
Conclusions: In our mixed ICU patient cohort, intra-abdominal hypertension occurred in almost half of all subjects and was twice as prevalent in mechanically ventilated patients as in spontaneously breathing patients. Presence and severity of intra-abdominal hypertension during the observation period significantly and independently increased 28- and 90-day mortality. Five admission day variables were independently associated with the presence or development of intra-abdominal hypertension. Positive fluid balance was associated with the development of intra-abdominal hypertension after day 1.
Figures

Comment in
-
Intra-Abdominal Hypertension in the ICU: Who to Measure? How to Prevent?Crit Care Med. 2019 Apr;47(4):608-609. doi: 10.1097/CCM.0000000000003675. Crit Care Med. 2019. PMID: 30882432 No abstract available.
References
-
- Malbrain ML, Cheatham ML, Kirkpatrick A, et al. Results from the international conference of experts on intra-abdominal hypertension and abdominal compartment syndrome. I. Definitions. Intensive Care Med 2006; 32:1722–1732 - PubMed
-
- Kirkpatrick AW, Roberts DJ, De Waele J, et al. ; Pediatric Guidelines Sub-Committee for the World Society of the Abdominal Compartment Syndrome: Intra-abdominal hypertension and the abdominal compartment syndrome: Updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med 2013; 39:1190–1206 - PMC - PubMed
-
- Kim IB, Prowle J, Baldwin I, et al. Incidence, risk factors and outcome associations of intra-abdominal hypertension in critically ill patients. Anaesth Intensive Care 2012; 40:79–89 - PubMed
-
- Iyer D, Rastogi P, Åneman A, et al. Early screening to identify patients at risk of developing intra-abdominal hypertension and abdominal compartment syndrome. Acta Anaesthesiol Scand 2014; 58:1267–1275 - PubMed
-
- Murphy PB, Parry NG, Sela N, et al. Intra-abdominal hypertension is more common than previously thought: A prospective study in a mixed medical-surgical ICU. Crit Care Med 2018; 46:958–964 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
