

Trigger finger secondary to a neglected flexor tendon rupture
- PMID: 30608439
- PMCID: PMC6344173
- DOI: 10.1097/MD.0000000000013980
Trigger finger secondary to a neglected flexor tendon rupture
Abstract
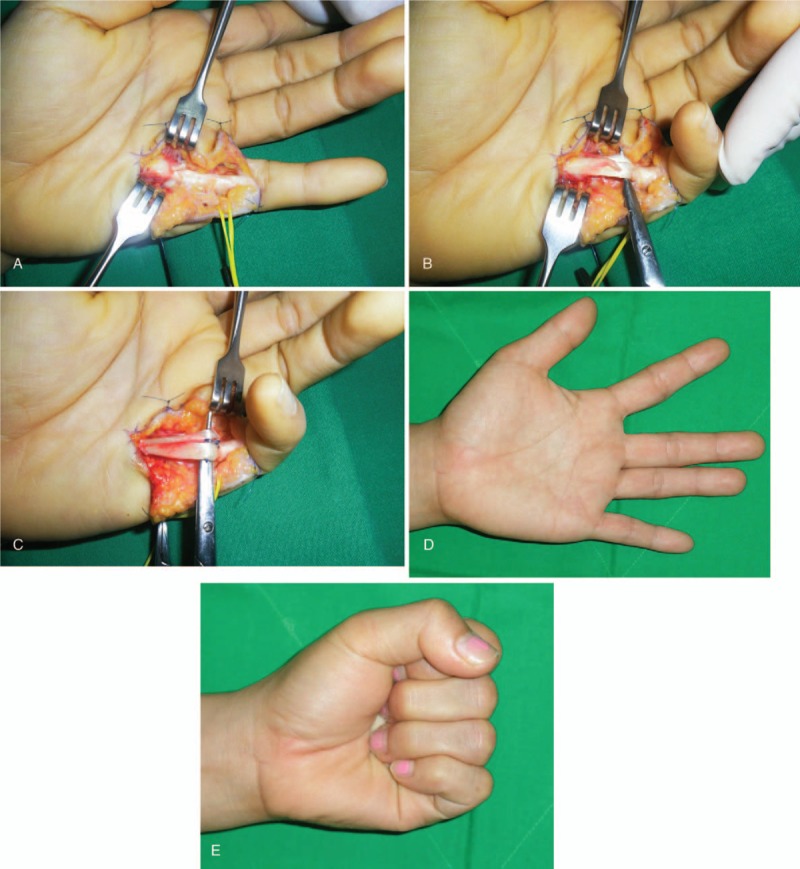
Secondary trigger finger caused by trauma to the hand, especially associated with partial flexor tendon rupture, is not a common condition. Thus, the clinical manifestations of these patients are not well-known. The aim of this study is to present secondary trigger finger caused by a neglected partial flexor tendon rupture including discussion of the mechanism and treatment.We retrospectively reviewed the records of 6 patients with trigger finger caused by a neglected partial flexor tendon rupture who had been treated with exploration, debridement, and repairing of the ruptured tendon from August 2010 to May 2015. The average patient age was 41 years (range, 23-59). The time from injury to treatment averaged 4.7 months. The average follow-up period was 9 months (range, 4-18). Functional outcome was evaluated from a comparison between the Quick-disabilities of the arm, shoulder, and hand (DASH) score and the visual analogue scale (VAS) for pain, which were measured at the time of preoperation and final follow up.Four patients showed partial rupture of the flexor digitorum profundus (FDP) tendon and 3 showed partial rupture of the flexor digitorun superficialis (FDS) tendon. Both the FDP and FDS tendons were partially ruptured in 2 patients, and the remaining patient had a partial rupture of the flexor pollicis longus tendon. All patients regained full range of motion, and there has been no recurrence of triggering. The average VAS score decreased from 3.6 (range, 3-5) preoperatively to 0.3 (range, 0-1) at the final follow up. The average Quick-DASH score decreased from 33.6 preoperatively to 5.3 at the final follow up.When we encounter patients with puncture or laceration wounds in flexor zone 2, even when the injury appears to be simple, partial flexor tendon laceration must be taken into consideration and early exploration is recommended.
Conflict of interest statement
All named authors hereby declare that they have no conflicts of interest to disclose.
Figures

References
-
- Weilby A. Trigger finger. Incidence in children and adults and the possibility of a predisposition in certain age group. Acta Orthop Scand 1970;41:419–27. - PubMed
-
- Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am 2006;31:135–46. - PubMed
-
- Wolfe SW. Green DP, Hotchkiss RN, Pederson WC. Tenosynovitis. Green's operative hand surgery. 5th ed.New York: Churchill Livingstone; 2005. 2137–58.
-
- Bilos ZJ, Hui PW, Stamelos S. Trigger finger following partial flexor tendon laceration. Hand 1977;9:232–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
