

Hospital Variation in the Utilization of Short-Term Nondurable Mechanical Circulatory Support in Myocardial Infarction Complicated by Cardiogenic Shock
- PMID: 30608880
- PMCID: PMC6424352
- DOI: 10.1161/CIRCINTERVENTIONS.118.007270
Hospital Variation in the Utilization of Short-Term Nondurable Mechanical Circulatory Support in Myocardial Infarction Complicated by Cardiogenic Shock
Abstract
Background: Limited knowledge exists on inter-hospital variation in the utilization of short-term, nondurable mechanical circulatory support (MCS) for myocardial infarction (MI) complicated by cardiogenic shock (CS).
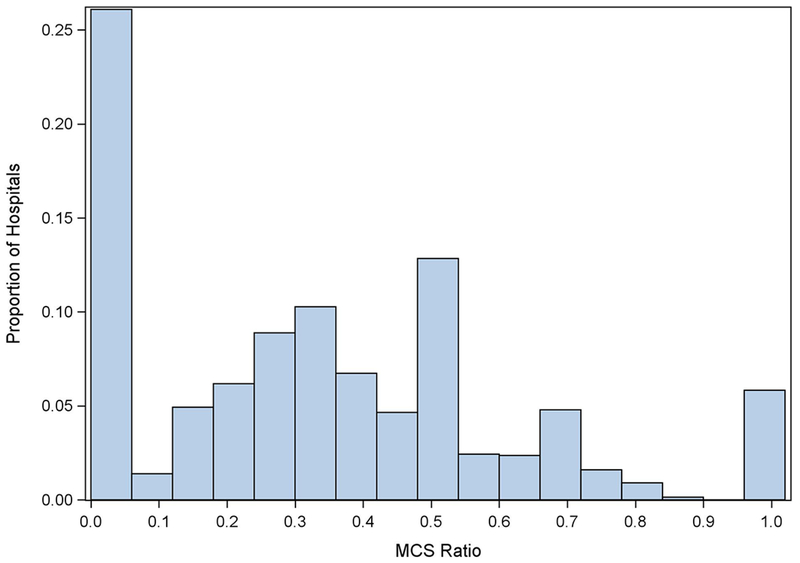
Methods and results: Hospitalizations for MI with CS in 2014 in a nationally representative all-payer database were included. The proportion of hospitalizations for MI with CS using MCS (MCS ratio) and in-hospital mortality were evaluated. Hospital characteristics and outcomes were compared across quartiles of MCS usage. Of 1813 hospitals evaluated, 1440 (79.4%) performed ≥10 percutaneous coronary interventions annually. Of these, 1064 (73.9%) had at least one code for MCS. Forty-one percent of hospitals did not use MCS. The median (interquartile range) proportion of MCS use among admissions for MI with CS was 33.3% (0.0%-50.0%). High MCS utilizing hospitals were larger ( P<0.001). Eighty-five percent (2808/3301) of MCS use was intra-aortic balloon pump. There was significant variation in receipt of MCS at different hospitals (median odds ratio of receiving MCS at 2 random hospitals: 1.58; 95% CI, 1.45-1.70). Adjusted in-hospital mortality was not different across quartiles of MCS use (Q4 versus Q1; odds ratio, 0.95; 95% CI, 0.77-1.16; P=0.58).
Conclusions: Wide variation exists in hospital use of MCS for MI with CS, unexplained by patient characteristics. The predominant form of MCS use is intra-aortic balloon pump. Risk-adjusted mortality rates were not different between higher and lower MCS-utilizing hospitals.
Keywords: critical care outcomes; intra-aortic balloon pumping; myocardial infarction; shock, cardiogenic.
Figures
References
-
- Adams KF Jr., Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, Berkowitz RL, Galvao M, Horton DP; ADHERE Scientific Advisory Committee and Investigators. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). American Heart Journal 2005;149:209–216. - PubMed
-
- Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS; NRMI Investigators. Trends in Management and Outcomes of Patients With Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA 2005;294:448. - PubMed
-
- Stretch R, Sauer CM, Yuh DD, Bonde P. National Trends in the Utilization of Short-Term Mechanical Circulatory Support. Journal of the American College of Cardiology 2014;64:1407–1415. - PubMed
-
- Strom JB, Zhao Y, Shen C, Chung M, Pinto DS, Popma JJ, Yeh RW. National Trends, Predictors of Use, and In-Hospital Outcomes in the Mechanical Circulatory Support for Cardiogenic Shock. EuroIntervention. 2018;13:e2152–e2159. - PubMed
-
- Bush M, Sturmer T, Stearns SC, Simpson RJ Jr, Brookhart MA, Rosamond W, Kucharska-Newton AM. Position matters: Validation of medicare hospital claims for myocardial infarction against medical record review in the atherosclerosis risk in communities study. Pharmacoepidemiol Drug Saf. 2018;27:1085–1091. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
