

Continuous and bolus intraventricular topotecan prolong survival in a mouse model of leptomeningeal medulloblastoma
- PMID: 30608927
- PMCID: PMC6319703
- DOI: 10.1371/journal.pone.0206394
Continuous and bolus intraventricular topotecan prolong survival in a mouse model of leptomeningeal medulloblastoma
Abstract
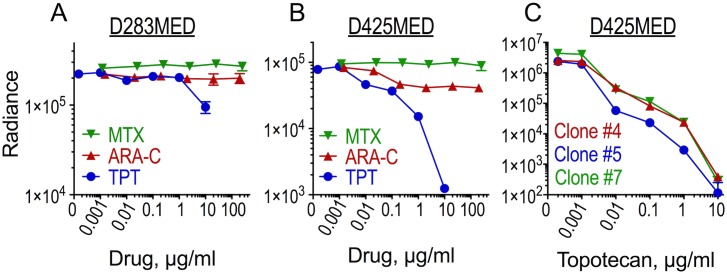
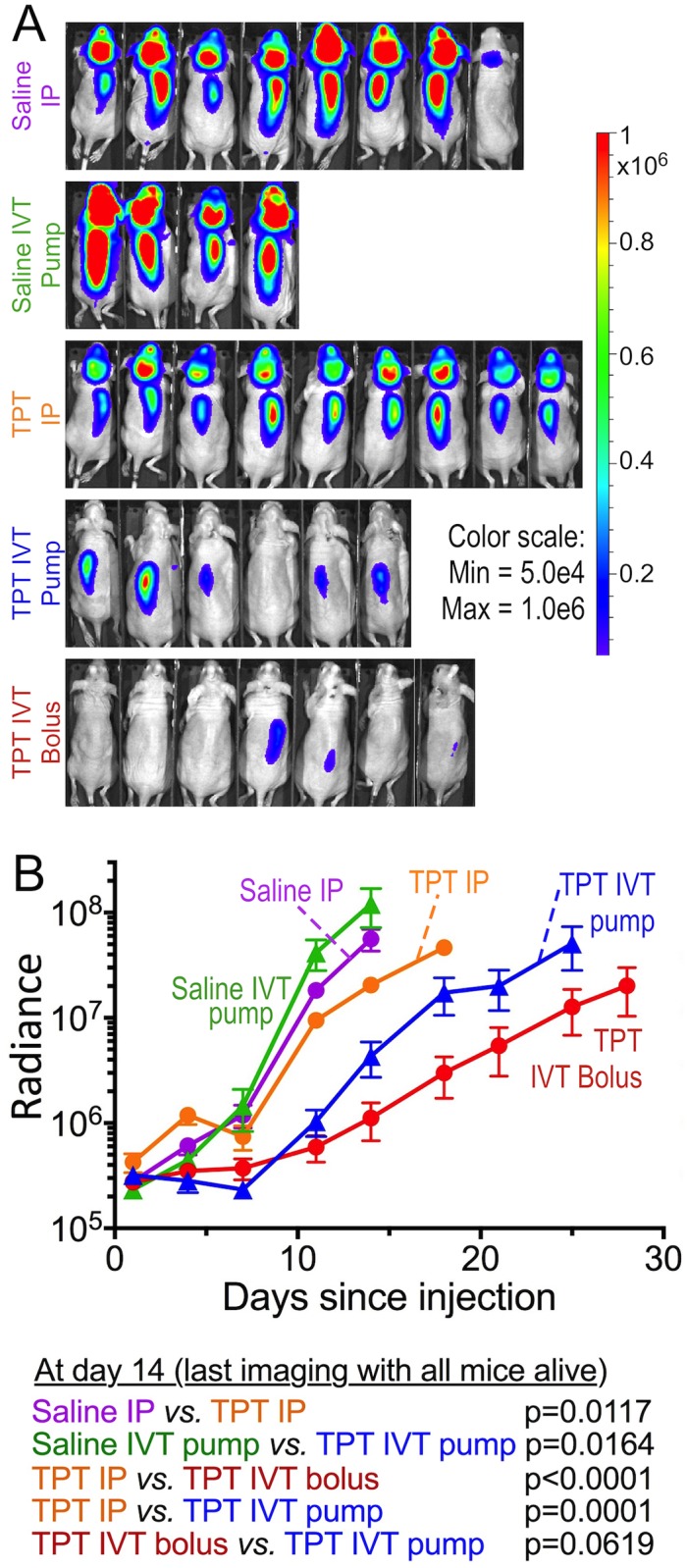
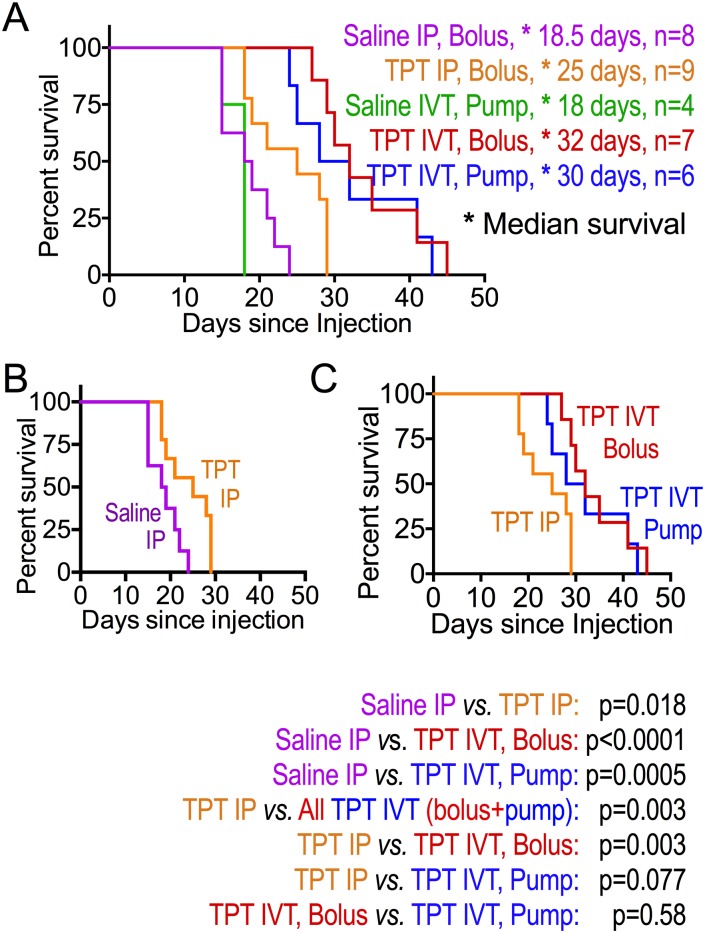
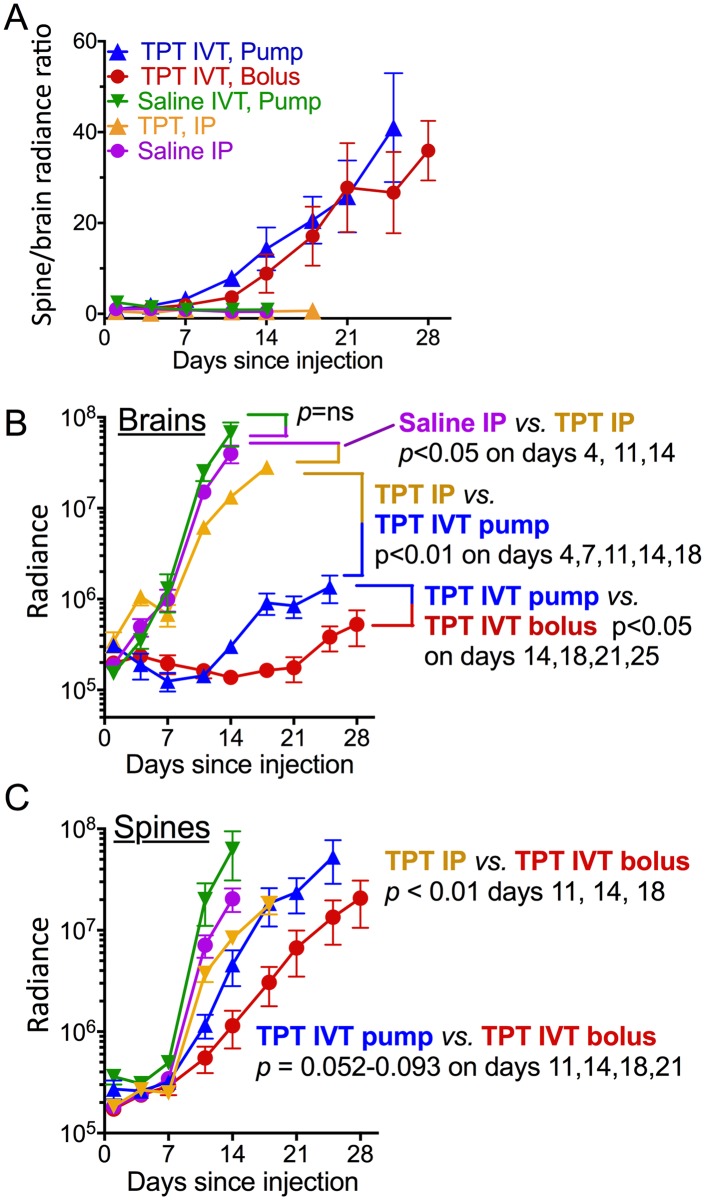
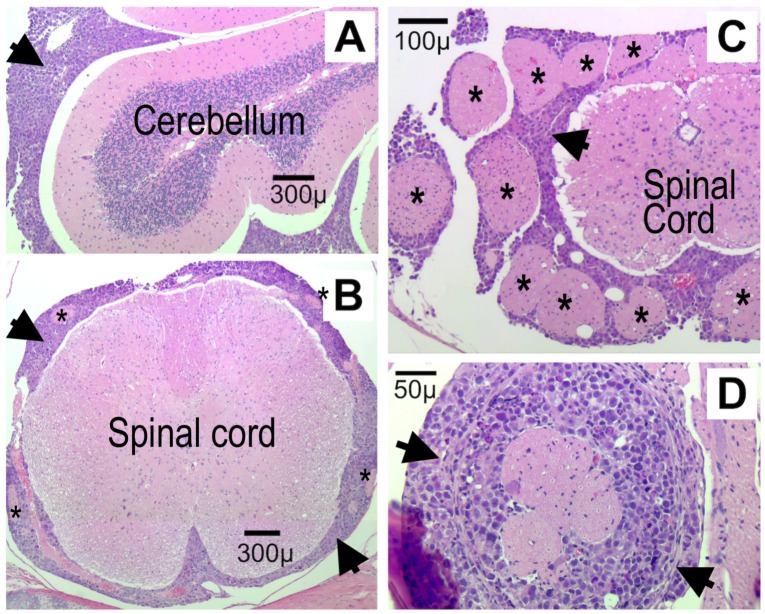
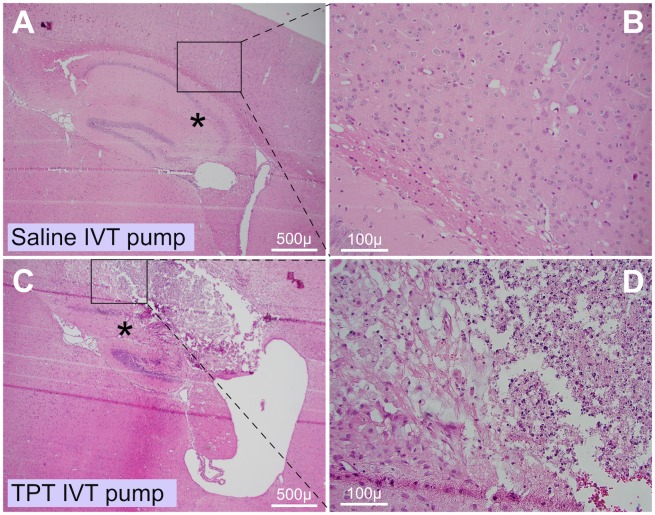
Leptomeningeal metastasis remains a difficult clinical challenge. Some success has been achieved by direct administration of therapeutics into the cerebrospinal fluid (CSF) circumventing limitations imposed by the blood brain barrier. Here we investigated continuous infusion versus bolus injection of therapy into the CSF in a preclinical model of human Group 3 medulloblastoma, the molecular subgroup with the highest incidence of leptomeningeal disease. Initial tests of selected Group 3 human medulloblastoma cell lines in culture showed that D283 Med and D425 Med were resistant to cytosine arabinoside and methotrexate. D283 Med cells were also resistant to topotecan, whereas 1 μM topotecan killed over 99% of D425 Med cells. We therefore introduced D425 Med cells, modified to express firefly luciferase, into the CSF of immunodeficient mice. Mice were then treated with topotecan or saline in five groups: continuous intraventricular (IVT) topotecan via osmotic pump (5.28 μg/day), daily bolus IVT topotecan injections with a similar daily dose (6 μg/day), systemic intraperitoneal injections of a higher daily dose of topotecan (15 μg/day), daily IVT pumped saline and daily intraperitoneal injections of saline. Bioluminescence analyses revealed that both IVT topotecan treatments effectively slowed leptomeningeal tumor growth in the brains. Histological analysis showed that they were associated with localized brain necrosis, possibly due to backtracking of topotecan around the catheter. In the spines, bolus IVT topotecan showed a trend towards slower tumor growth compared to continuous (pump) IVT topotecan, as measured by bioluminescence. Both continuous and bolus topotecan IVT showed longer survival compared to other groups. Thus, both direct IVT topotecan CSF delivery methods produced better anti-medulloblastoma effect compared to systemic therapy at the dosages used here.
Conflict of interest statement
EM and TH have a financial interest in Fluid Synchrony LLC. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Pilot study assessing a seven-day continuous intrathecal topotecan infusion for recurrent or progressive leptomeningeal metastatic cancer.J Oncol Pharm Pract. 2014 Jun;20(3):229-32. doi: 10.1177/1078155213494940. Epub 2013 Aug 8. J Oncol Pharm Pract. 2014. PMID: 23929729
-
Intra-CSF topotecan in treatment of breast cancer patients with leptomeningeal metastases.Cancer Med. 2020 Nov;9(21):7935-7942. doi: 10.1002/cam4.3422. Epub 2020 Sep 3. Cancer Med. 2020. PMID: 32885617 Free PMC article.
-
Valproic Acid prolongs survival time of severe combined immunodeficient mice bearing intracerebellar orthotopic medulloblastoma xenografts.Clin Cancer Res. 2006 Aug 1;12(15):4687-94. doi: 10.1158/1078-0432.CCR-05-2849. Clin Cancer Res. 2006. PMID: 16899619
-
Pharmacokinetics following intraventricular administration of chemotherapy in patients with neoplastic meningitis.Clin Pharmacokinet. 2005;44(1):1-31. doi: 10.2165/00003088-200544010-00001. Clin Pharmacokinet. 2005. PMID: 15634030 Review.
-
A review of leptomeningeal metastases in pediatrics.J Child Neurol. 1995 May;10(3):191-9. doi: 10.1177/088307389501000304. J Child Neurol. 1995. PMID: 7642887 Review.
Cited by
-
A Murine Ommaya Xenograft Model to Study Direct-Targeted Therapy of Leptomeningeal Disease.J Vis Exp. 2021 Jan 29;(167):10.3791/62033. doi: 10.3791/62033. J Vis Exp. 2021. PMID: 33586709 Free PMC article.
-
The OTX2 Gene Induces Tumor Growth and Triggers Leptomeningeal Metastasis by Regulating the mTORC2 Signaling Pathway in Group 3 Medulloblastomas.Int J Mol Sci. 2024 Apr 17;25(8):4416. doi: 10.3390/ijms25084416. Int J Mol Sci. 2024. PMID: 38674001 Free PMC article.
-
Beyond the brain: exploring the impact of animal models of leptomeningeal disease from solid tumors.Acta Neuropathol Commun. 2025 May 19;13(1):103. doi: 10.1186/s40478-025-01959-4. Acta Neuropathol Commun. 2025. PMID: 40383789 Free PMC article. Review.
-
The path to leptomeningeal metastasis.Nat Rev Cancer. 2024 Jul;24(7):448-460. doi: 10.1038/s41568-024-00700-y. Epub 2024 Jun 13. Nat Rev Cancer. 2024. PMID: 38871881 Free PMC article. Review.
References
-
- Fouladi M, Gajjar A, Boyett JM, Walter AW, Thompson SJ, et al. (1999) Comparison of CSF cytology and spinal magnetic resonance imaging in the detection of leptomeningeal disease in pediatric medulloblastoma or primitive neuroectodermal tumor. J Clin Oncol 17: 3234–3237. 10.1200/JCO.1999.17.10.3234 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
