

High prevalence of nonalcoholic steatohepatitis and abnormal liver stiffness in a young and obese Mexican population
- PMID: 30608932
- PMCID: PMC6319733
- DOI: 10.1371/journal.pone.0208926
High prevalence of nonalcoholic steatohepatitis and abnormal liver stiffness in a young and obese Mexican population
Abstract
Objective: To identify nonalcoholic steatohepatitis (NASH) and liver stiffness in Mexican subjects with different body mass index (BMI).
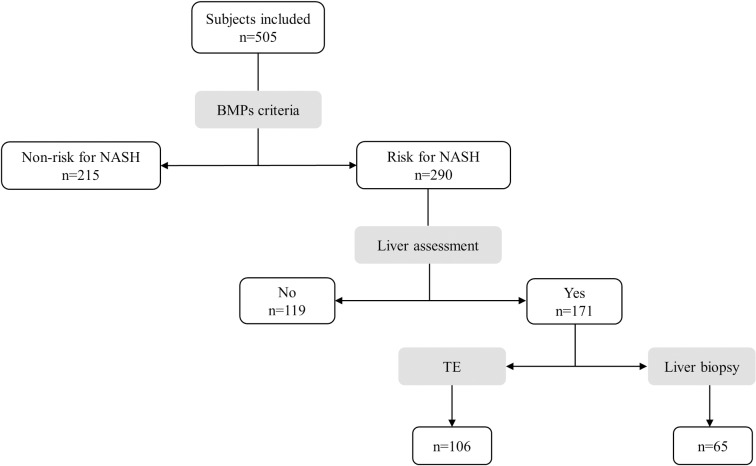
Methods: A cross-sectional study was conducted in 505 adults. Risk for NASH was defined as the presence of one or more of the following biochemical and metabolic parameters (BMPs): fasting glucose ≥100 mg/dl, triglycerides (TG) ≥150 mg/dl, homeostatic model assessment of insulin resistance (HOMA-IR) ≥2.5, aspartate aminotransferase (AST) >54 IU/L and alanine aminotransferase (ALT) >42 IU/L. Body mass index measurement and nutritional assessment were performed by standard procedures. Liver fibrosis stage was determined by liver stiffness measurement using transitional elastography (TE) or by liver biopsy (LB).
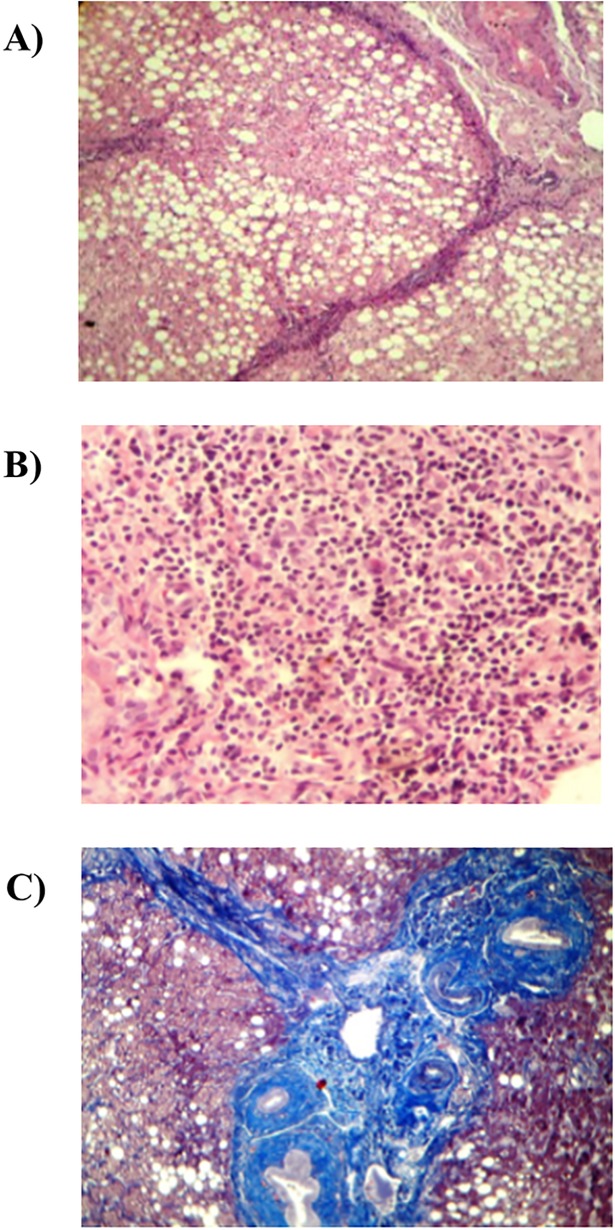
Results: Risk for NASH was 57% (290/505). Most BMPs values incremented by BMI category. Among 171 at-risk patients, 106 subjects were evaluated by TE and 65 subjects by LB. Abnormal liver stiffness (≥6.0 kPa) was prevalent in 54% (57/106) of the cases, whereas by LB, 91% (59/65) of patients with obesity had NASH and liver fibrosis. Furthermore, liver fibrosis was prevalent in 46% (6/13) in normal weight individuals, whereas 4.6% (3/65) of patients with a BMI ≥ 35 kg/m2 showed no histopathological abnormalities. Overall, 67.8% (116/171) of the patients had abnormal liver stiffness or NASH. The normal weight patients with liver damage consumed relatively a higher fat-rich diet compared to the other groups whereas the remaining subgroups shared a similar dietary pattern.
Conclusion: Young patients with overweight and obesity showed a high prevalence of altered BMPs related to abnormal liver stiffness assessed by TE and NASH by LB. Early diagnostic strategies are required to detect the risk for NASH and avoid further liver damage in populations with a rising prevalence of obesity by defining the risk factors involved in the onset and progression of NASH.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Global Burden of Disease Liver Cancer Collaboration, Akinyemiju T, Abera S, Ahmed M, Alam N, Alemayohu MA, et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017; 3:1683–1691. 10.1001/jamaoncol.2017.3055 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
