

Diagnostic yield of genetic tests in epilepsy: A meta-analysis and cost-effectiveness study
- PMID: 30610098
- PMCID: PMC6369901
- DOI: 10.1212/WNL.0000000000006850
Diagnostic yield of genetic tests in epilepsy: A meta-analysis and cost-effectiveness study
Abstract
Objective: To compare the cost-effectiveness of genetic testing strategies in patients with epilepsy of unknown etiology.
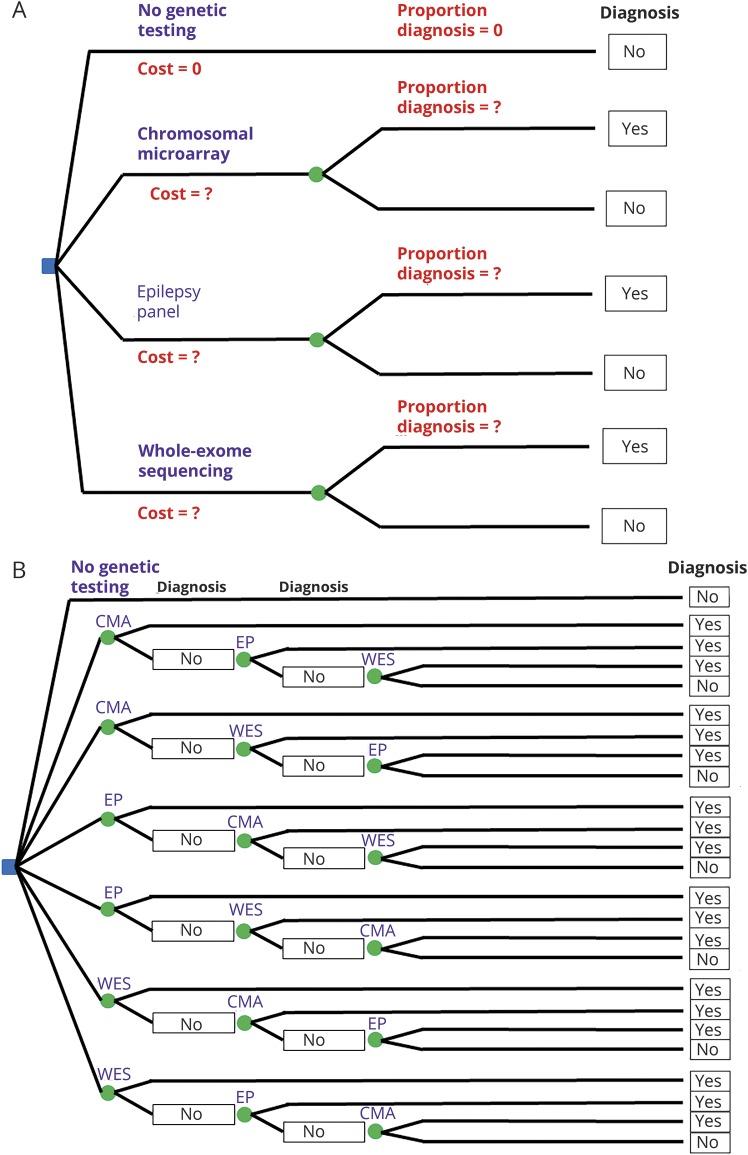
Methods: This meta-analysis and cost-effectiveness study compared strategies involving 3 genetic tests: chromosomal microarray (CMA), epilepsy panel (EP) with deletion/duplication testing, and whole-exome sequencing (WES) in a cost-effectiveness model, using "no genetic testing" as a point of comparison.
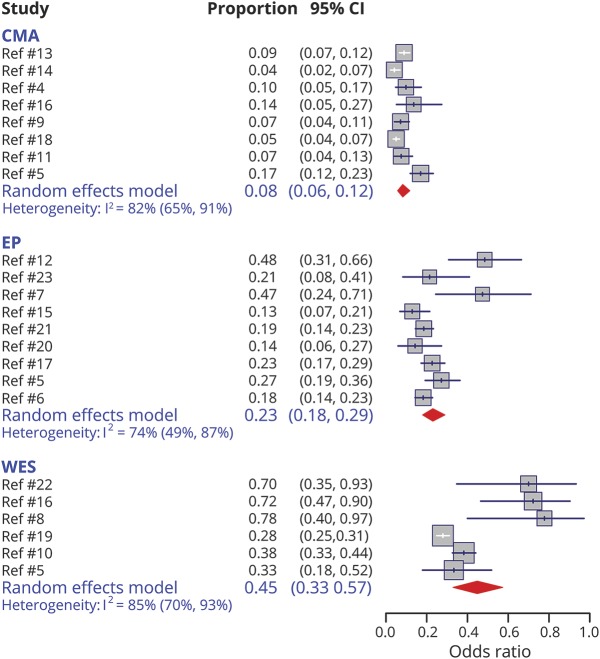
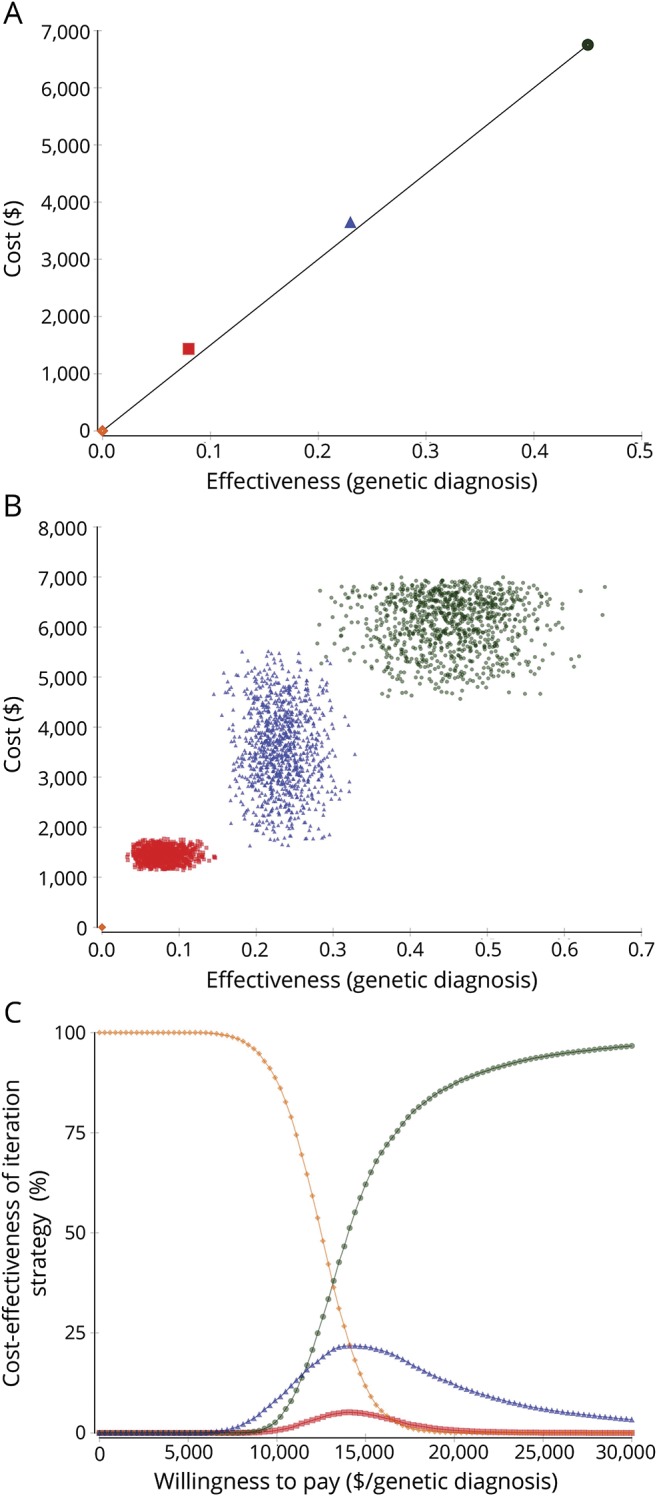
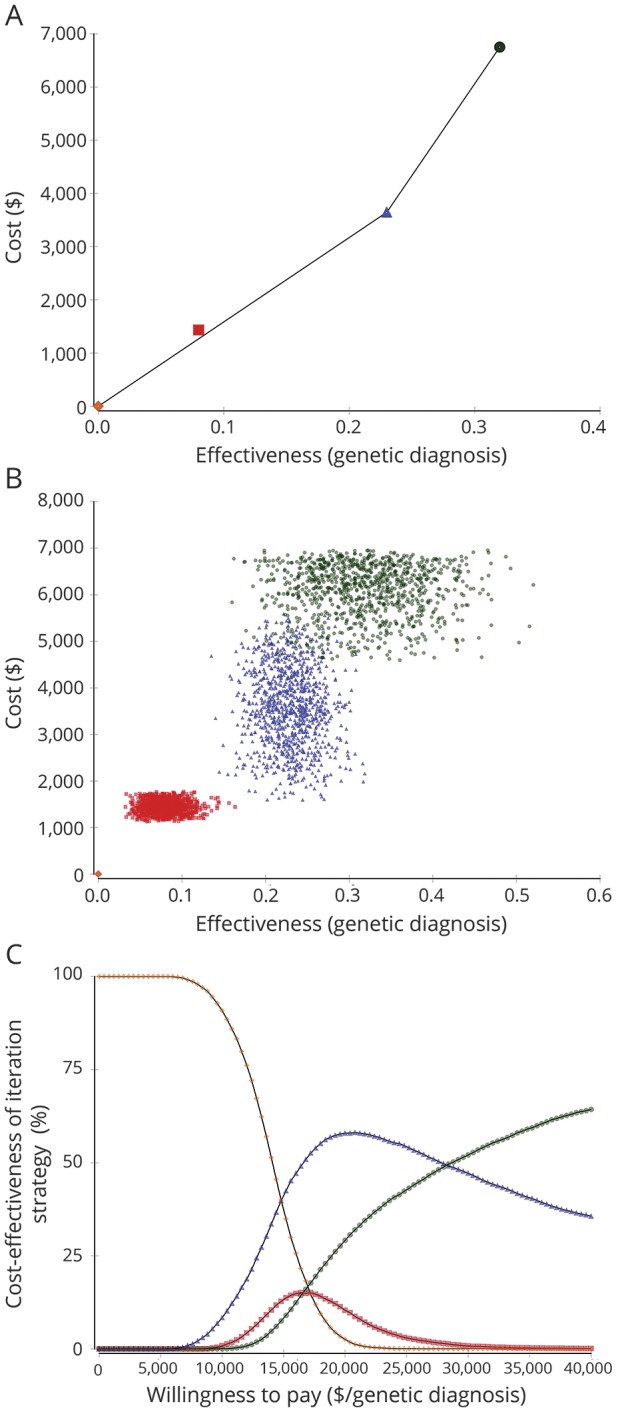
Results: Twenty studies provided information on the diagnostic yield of CMA (8 studies), EP (9 studies), and WES (6 studies). The diagnostic yield was highest for WES: 0.45 (95% confidence interval [CI]: 0.33-0.57) (0.32 [95% CI: 0.22-0.44] adjusting for potential publication bias), followed by EP: 0.23 (95% CI: 0.18-0.29), and CMA: 0.08 (95% CI: 0.06-0.12). The most cost-effective test was WES with an incremental cost-effectiveness ratio (ICER) of $15,000/diagnosis. However, after adjusting for potential publication bias, the most cost-effective test was EP (ICER: $15,848/diagnosis) followed by WES (ICER: $34,500/diagnosis). Among combination strategies, the most cost-effective strategy was WES, then if nondiagnostic, EP, then if nondiagnostic, CMA (ICER: $15,336/diagnosis), although adjusting for potential publication bias, the most cost-effective strategy was EP ± CMA ± WES (ICER: $18,385/diagnosis). While the cost-effectiveness of individual tests and testing strategies overlapped, CMA was consistently less cost-effective than WES and EP.
Conclusion: WES and EP are the most cost-effective genetic tests for epilepsy. Our analyses support, for a broad population of patients with unexplained epilepsy, starting with these tests. Although less expensive, CMA has lower yield, and its use as the first-tier test is thus not supported from a cost-effectiveness perspective.
© 2019 American Academy of Neurology.
Figures
Comment in
-
The Road to Diagnosis: Shortening the Diagnostic Odyssey in Epilepsy.Epilepsy Curr. 2019 Sep;19(5):307-309. doi: 10.1177/1535759719871593. Epub 2019 Sep 2. Epilepsy Curr. 2019. PMID: 31476917 Free PMC article.
References
-
- Forsgren L, Beghi E, Oun A, Sillanpaa M. The epidemiology of epilepsy in Europe: a systematic review. Eur J Neurol 2005;12:245–253. - PubMed
-
- Hauser WA, Annegers JF, Rocca WA. Descriptive epidemiology of epilepsy: contributions of population-based studies from Rochester, Minnesota. Mayo Clin Proc 1996;71:576–586. - PubMed
-
- Thomas RH, Berkovic SF. The hidden genetics of epilepsy: a clinically important new paradigm. Nat Rev Neurol 2014;10:283–292. - PubMed
-
- Bartnik M, Szczepanik E, Derwinska K, et al. Application of array comparative genomic hybridization in 102 patients with epilepsy and additional neurodevelopmental disorders. Am J Med Genet B Neuropsychiatr Genet 2012;159B:760–771. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical