

Outcomes and Risk Score for Distal Pancreatectomy with Celiac Axis Resection (DP-CAR): An International Multicenter Analysis
- PMID: 30610560
- PMCID: PMC6373251
- DOI: 10.1245/s10434-018-07101-0
Outcomes and Risk Score for Distal Pancreatectomy with Celiac Axis Resection (DP-CAR): An International Multicenter Analysis
Abstract
Background: Distal pancreatectomy with celiac axis resection (DP-CAR) is a treatment option for selected patients with pancreatic cancer involving the celiac axis. A recent multicenter European study reported a 90-day mortality rate of 16%, highlighting the importance of patient selection. The authors constructed a risk score to predict 90-day mortality and assessed oncologic outcomes.
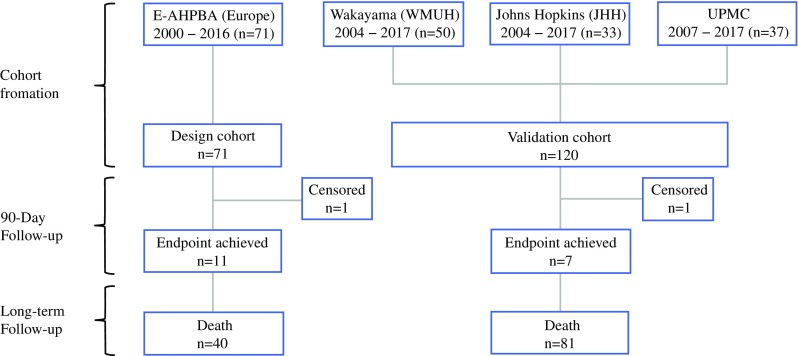
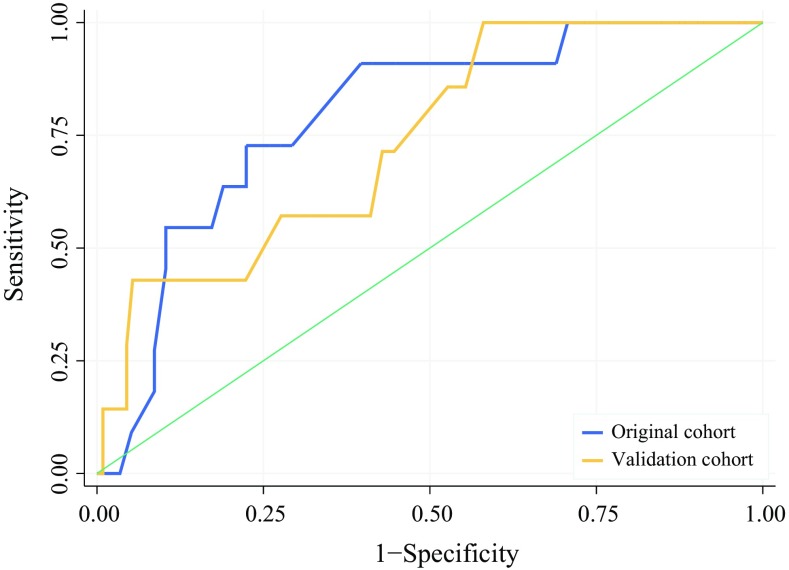
Methods: This multicenter retrospective cohort study investigated patients undergoing DP-CAR at 20 European centers from 12 countries (model design 2000-2016) and three very-high-volume international centers in the United States and Japan (model validation 2004-2017). The area under receiver operator curve (AUC) and calibration plots were used for validation of the 90-day mortality risk model. Secondary outcomes included resection margin status, adjuvant therapy, and survival.
Results: For 191 DP-CAR patients, the 90-day mortality rate was 5.5% (95 confidence interval [CI], 2.2-11%) at 5 high-volume (≥ 1 DP-CAR/year) and 18% (95 CI, 9-30%) at 18 low-volume DP-CAR centers (P = 0.015). A risk score with age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, multivisceral resection, open versus minimally invasive surgery, and low- versus high-volume center performed well in both the design and validation cohorts (AUC, 0.79 vs 0.74; P = 0.642). For 174 patients with pancreatic ductal adenocarcinoma, the R0 resection rate was 60%, neoadjuvant and adjuvant therapies were applied for respectively 69% and 67% of the patients, and the median overall survival period was 19 months (95 CI, 15-25 months).
Conclusions: When performed for selected patients at high-volume centers, DP-CAR is associated with acceptable 90-day mortality and overall survival. The authors propose a 90-day mortality risk score to improve patient selection and outcomes, with DP-CAR volume as the dominant predictor.
Figures
References
-
- Kondo S, Katoh H, Shimizu T, et al. Preoperative embolization of the common hepatic artery in preparation for radical pancreatectomy for pancreas body cancer. Hepatogastroenterology. 2000;47:1447–1449. - PubMed
-
- Ocuin LM, Miller-Ocuin JL, Novak SM, et al. Robotic and open distal pancreatectomy with celiac axis resection for locally advanced pancreatic body tumors: a single-institutional assessment of perioperative outcomes and survival. HPB. 2016;18:835–842. doi: 10.1016/j.hpb.2016.05.003. - DOI - PMC - PubMed
-
- Nakamura T, Hirano S, Noji T, et al. Distal pancreatectomy with en bloc celiac axis resection (modified appleby procedure) for locally advanced pancreatic body cancer: a single-center review of 80 consecutive patients. Ann Surg Oncol. 2016;23(Suppl 5):969–975. doi: 10.1245/s10434-016-5493-8. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
