

Evaluation of stereotactic radiosurgery for cerebral dural arteriovenous fistulas in a multicenter international consortium
- PMID: 30611144
- PMCID: PMC6609496
- DOI: 10.3171/2018.8.JNS181467
Evaluation of stereotactic radiosurgery for cerebral dural arteriovenous fistulas in a multicenter international consortium
Abstract
Objective: In this multicenter study, the authors reviewed the results obtained in patients who underwent Gamma Knife radiosurgery (GKRS) for dural arteriovenous fistulas (dAVFs) and determined predictors of outcome.
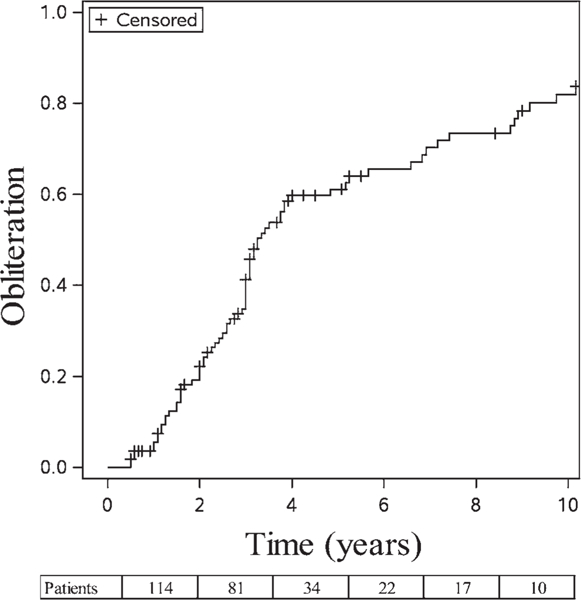
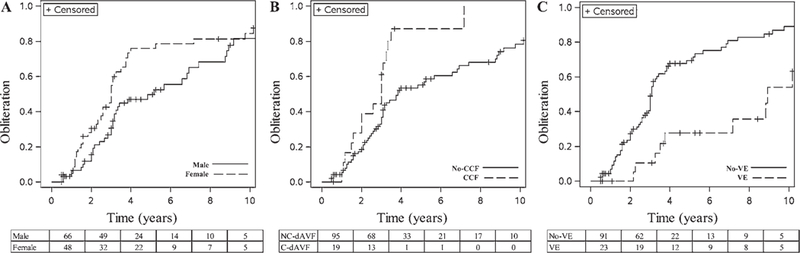
Methods: Data from a cohort of 114 patients who underwent GKRS for cerebral dAVFs were compiled from the International Gamma Knife Research Foundation. Favorable outcome was defined as dAVF obliteration and no posttreatment hemorrhage or permanent symptomatic radiation-induced complications. Patient and dAVF characteristics were assessed to determine predictors of outcome in a multivariate logistic regression analysis; dAVF-free obliteration was calculated in a competing-risk survival analysis; and Youden indices were used to determine optimal radiosurgical dose.
Results: A mean margin dose of 21.8 Gy was delivered. The mean follow-up duration was 4 years (range 0.5-18 years). The overall obliteration rate was 68.4%. The postradiosurgery actuarial rates of obliteration at 3, 5, 7, and 10 years were 41.3%, 61.1%, 70.1%, and 82.0%, respectively. Post-GRKS hemorrhage occurred in 4 patients (annual risk of 0.9%). Radiation-induced imaging changes occurred in 10.4% of patients; 5.2% were symptomatic, and 3.5% had permanent deficits. Favorable outcome was achieved in 63.2% of patients. Patients with middle fossa and tentorial dAVFs (OR 2.4, p = 0.048) and those receiving a margin dose greater than 23 Gy (OR 2.6, p = 0.030) were less likely to achieve a favorable outcome. Commonly used grading scales (e.g., Borden and Cognard) were not predictive of outcome. Female sex (OR 1.7, p = 0.03), absent venous ectasia (OR 3.4, p < 0.001), and cavernous carotid location (OR 2.1, p = 0.019) were predictors of GKRS-induced dAVF obliteration.
Conclusions: GKRS for cerebral dAVFs achieved obliteration and avoided permanent complications in the majority of patients. Those with cavernous carotid location and no venous ectasia were more likely to have fistula obliteration following radiosurgery. Commonly used grading scales were not reliable predictors of outcome following radiosurgery.
Keywords: C-dAVF = cavernous dAVF; CVD = cortical venous drainage; GKRS = Gamma Knife radiosurgery; Gamma Knife; ICH = intracerebral hemorrhage; RIC = radiation-induced complication; SAH = subarachnoid hemorrhage; arteriovenous; dAVF = dural arteriovenous fistula; dural; fistula; outcome; stereotactic radiosurgery; vascular disorders.
Figures
References
-
- Altman DG: Practical Statistics for Medical Research. Boca Raton, FL: CRC Press, 1990
-
- Borden JA, Wu JK, Shucart WA: A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg 82:166–179, 1995 - PubMed
-
- Bulters DO, Mathad N, Culliford D, Millar J, Sparrow OC: The natural history of cranial dural arteriovenous fistulae with cortical venous reflux—the significance of venous ectasia. Neurosurgery 70:312–319, 2012 - PubMed
-
- Chaichana KL, Coon AL, Tamargo RJ, Huang J: Dural arteriovenous fistulas: epidemiology and clinical presentation. Neurosurg Clin N Am 23:7–13, 2012 - PubMed
-
- Chen CJ, Lee CC, Ding D, Starke RM, Chivukula S, Yen CP, et al.: Stereotactic radiosurgery for intracranial dural arteriovenous fistulas: a systematic review. J Neurosurg 122:353–362, 2015 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
