

The Effects of Hepatitis C Treatment Eligibility Criteria on All-cause Mortality Among People With Human Immunodeficiency Virus
- PMID: 30615096
- PMCID: PMC6792128
- DOI: 10.1093/cid/ciz008
The Effects of Hepatitis C Treatment Eligibility Criteria on All-cause Mortality Among People With Human Immunodeficiency Virus
Abstract
Background: The cost of direct-acting antivirals (DAAs) for hepatitis C virus (HCV) prompted many payers to restrict treatment to patients who met non-evidence-based criteria. These restrictions have implications for survival of people with HCV, especially for people with human immunodeficiency virus (HIV)/HCV coinfection who are at high risk for liver disease progression. The goal of this work was to estimate the effects of DAA access policies on 10-year all-cause mortality among people with HIV.
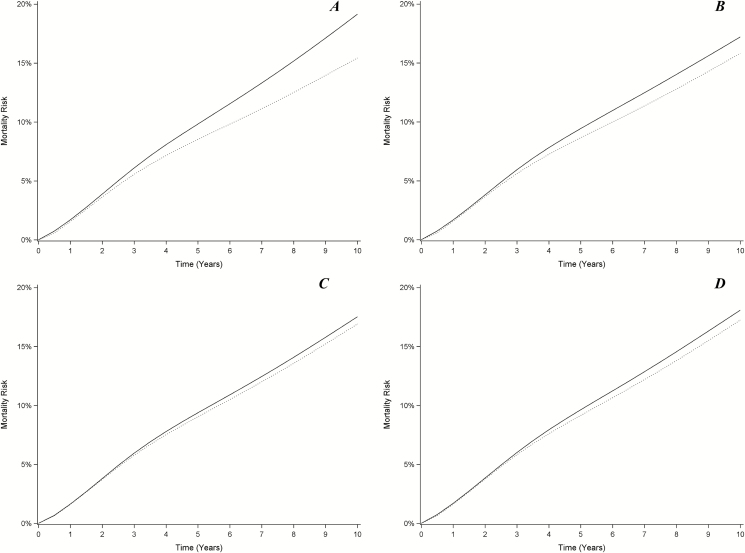
Methods: The study population included 3056 adults with HIV in the Women's Interagency HIV Study and Multicenter AIDS Cohort Study from 1 October 1994 through 30 September 2015. We used the parametric g-formula to estimate 10-year all-cause mortality under DAA access policies that included treating (i) all people with HCV; (ii) only people with suppressed HIV; (iii) only people with severe fibrosis; and (iv) only people with HIV suppression and severe fibrosis.
Results: The 10-year risk difference of treating all coinfected persons with DAAs compared with no treatment was -3.7% (95% confidence interval [CI], -9.1% to .6%). Treating only those with suppressed HIV and severe fibrosis yielded a risk difference of -1.1% (95% CI, -2.8% to .6%), with 51% (95% CI, 38%-59%) of coinfected persons receiving DAAs. Treating a random selection of 51% of coinfected persons at baseline decreased the risk by 1.9% (95% CI, -4.7% to .3%).
Conclusions: Restrictive DAA access policies may decrease survival compared to treating similar proportions of people with HIV/HCV coinfection with DAAs at random. These findings suggest that lives could be saved by thoughtfully revising access policies.
Keywords: antiretroviral therapy; direct-acting antivirals; hepatitis C virus; human immunodeficiency virus; population intervention effects.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Collins S, Mertenskoetter T, Loeliger E, et al. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D Study. Arch Intern Med 2006; 166:1632–41. - PubMed
-
- Weber R, Ruppik M, Rickenbach M, et al. Swiss HIV Cohort Study Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med 2013; 14:195–207. - PubMed
-
- Milazzo L, Lai A, Calvi E, et al. Direct-acting antivirals in hepatitis C virus (HCV)-infected and HCV/HIV-coinfected patients: real-life safety and efficacy. HIV Med 2017; 18:284–91. - PubMed
-
- National Viral Hepatitis Roundtable, Harvard Law School Center for Health Law and Policy Innovation. Hepatitis C: the state of Medicaid access. 2017. Available at: https://stateofhepc.org/wp-content/uploads/2017/10/State-of-HepC_2017_FI.... Accessed 2 April 2018.
-
- Ooka K, Connolly JJ, Lim JK. Medicaid reimbursement for oral direct antiviral agents for the treatment of chronic hepatitis C. Am J Gastroenterol 2017; 112:828–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI035042/AI/NIAID NIH HHS/United States
- R38 AI140299/AI/NIAID NIH HHS/United States
- U01 AI103397/AI/NIAID NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- K24 AI108516/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 HL146242/HL/NHLBI NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- R01 AI100654/AI/NIAID NIH HHS/United States
- U01 HL146194/HL/NHLBI NIH HHS/United States
- U54 AG062334/AG/NIA NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- DP2 HD084070/HD/NICHD NIH HHS/United States
- U01 HL146205/HL/NHLBI NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- R21 AG059505/AG/NIA NIH HHS/United States
- U01 AI103390/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- U01 HL146203/HL/NHLBI NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
