

Incidence and Mortality of Acute-on-Chronic Liver Failure Using Two Definitions in Patients with Compensated Cirrhosis
- PMID: 30615211
- PMCID: PMC6461492
- DOI: 10.1002/hep.30494
Incidence and Mortality of Acute-on-Chronic Liver Failure Using Two Definitions in Patients with Compensated Cirrhosis
Abstract
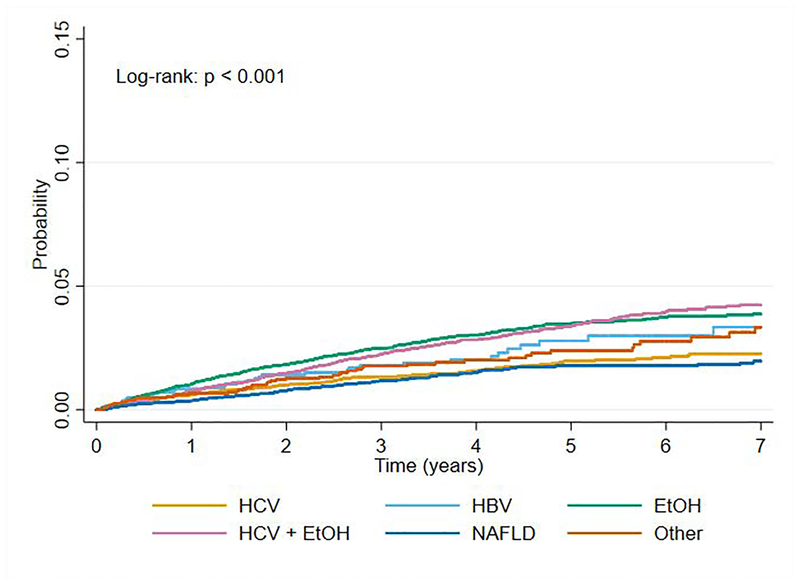
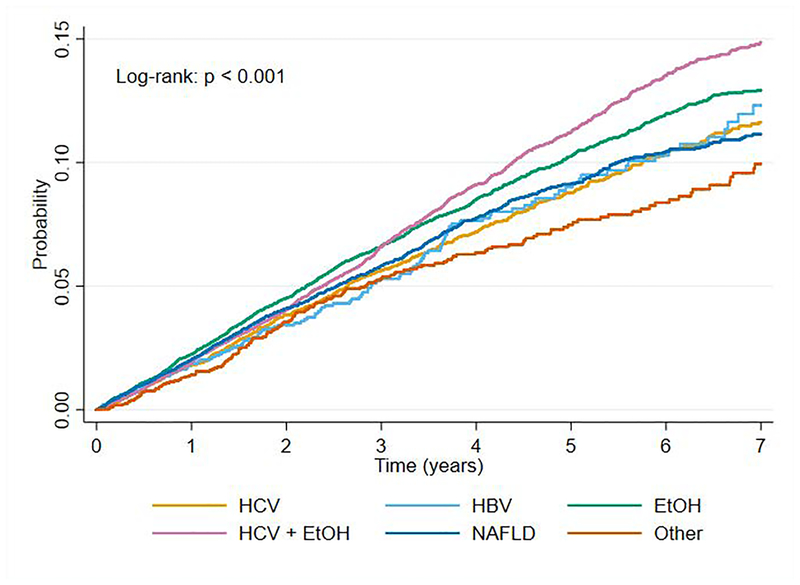
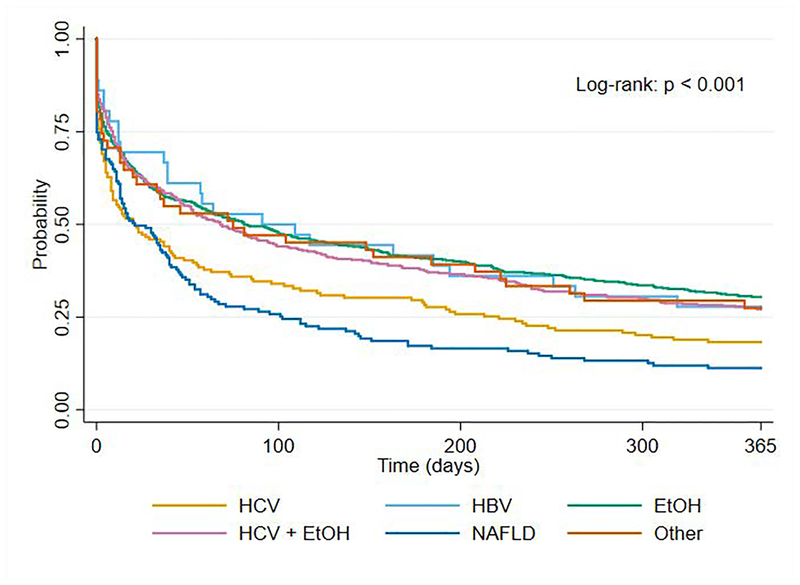
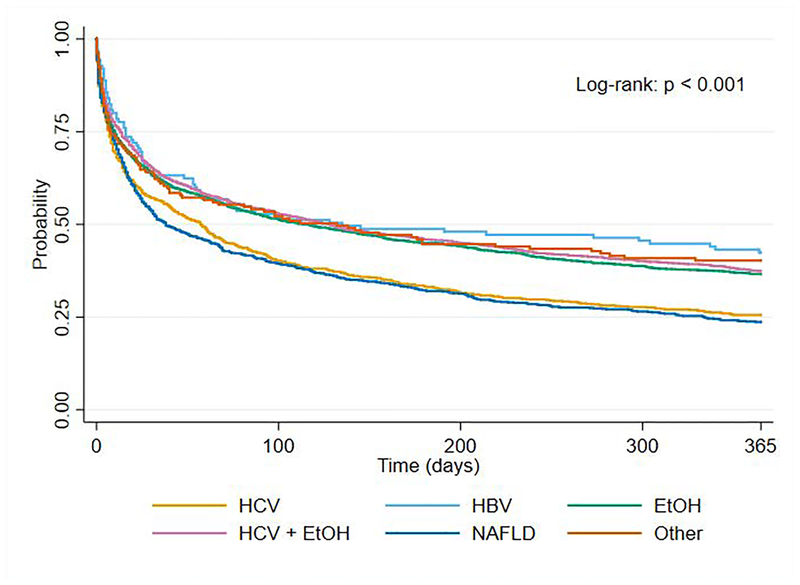
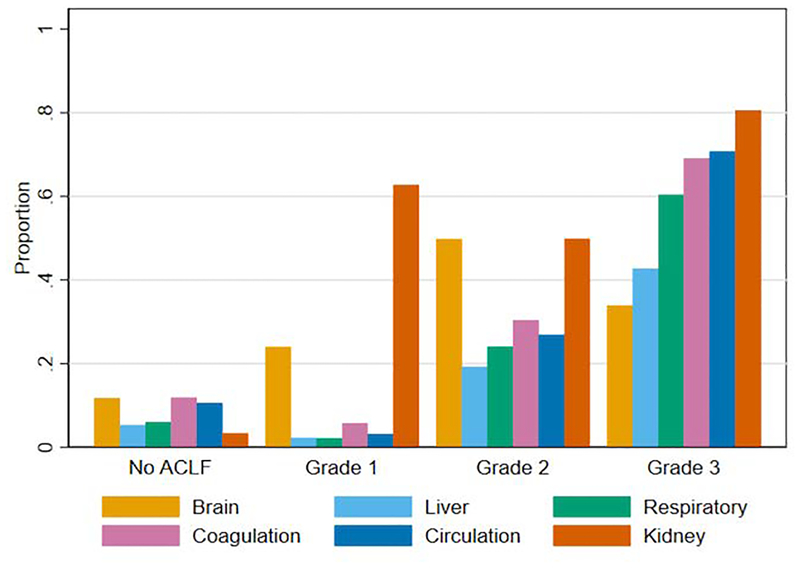
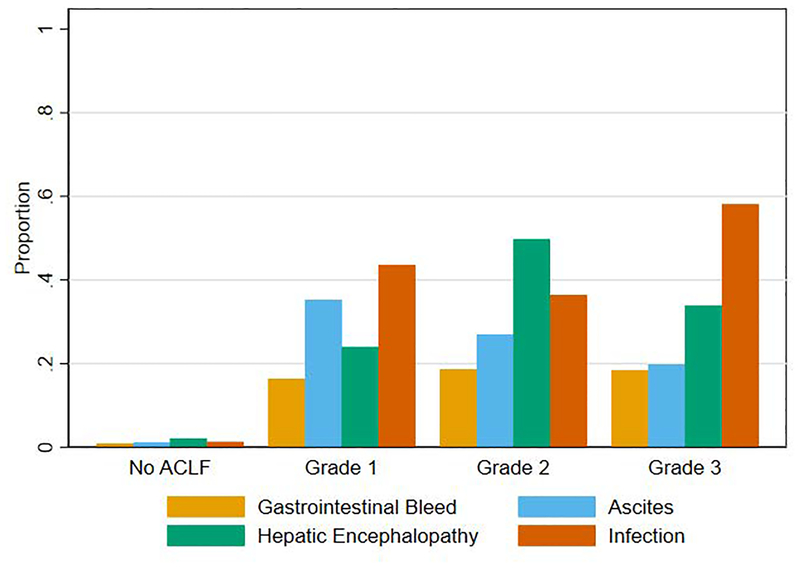
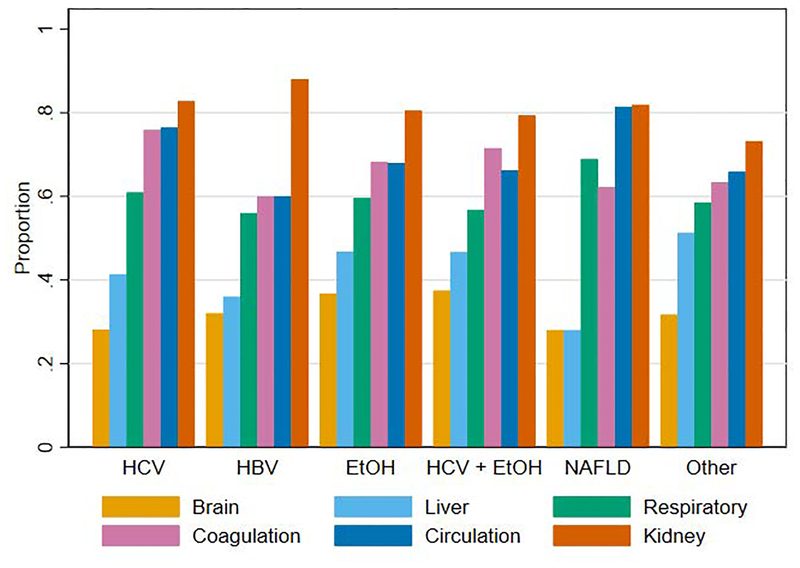
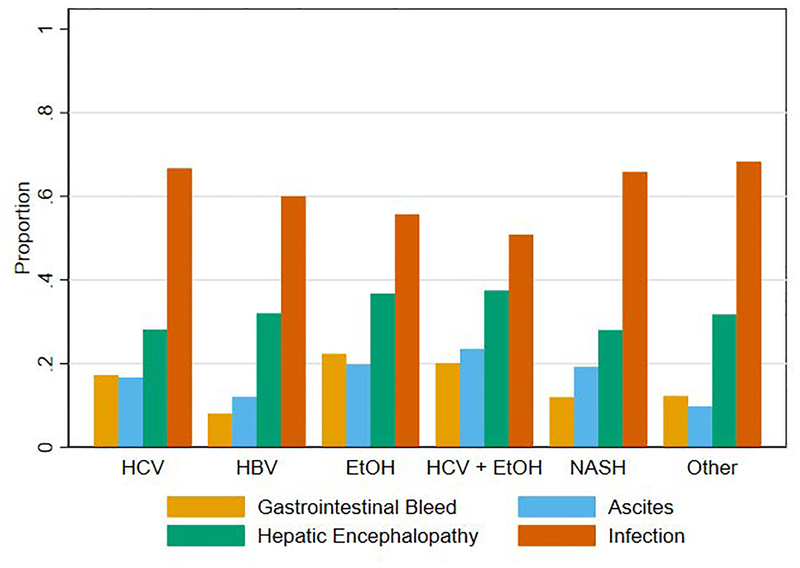
The term acute-on-chronic liver failure (ACLF) is intended to identify patients with chronic liver disease who develop rapid deterioration of liver function and high short-term mortality after an acute insult. The two prominent definitions (European Association for the Study of the Liver [EASL] and Asian Pacific Association for the Study of the Liver [APASL]) differ, and existing literature applies to narrow patient groups. We sought to compare ACLF incidence and mortality among a diverse cohort of patients with compensated cirrhosis, using both definitions. This was a retrospective cohort study of patients with incident compensated cirrhosis in the Veterans Health Administration from 2008 to 2016. First ACLF events were identified for each definition. Incidence rates were computed as events per 1,000 person-years, and mortality was calculated at 28 and 90 days. Among 80,383 patients with cirrhosis with 3.35 years median follow-up, 783 developed EASL and APASL ACLF, 4,296 developed EASL ACLF alone, and 574 developed APASL ACLF alone. The incidence rate of APASL ACLF was 5.7 per 1,000 person-years (95% confidence interval [CI]: 5.4-6.0), and the incidence rate of EASL ACLF was 20.1 (95% CI: 19.5-20.6). The 28-day and 90-day mortalities for APASL ACLF were 41.9% and 56.1%, respectively, and were 37.6% and 50.4% for EASL ACLF. The median bilirubin level at diagnosis of EASL-alone ACLF was 2.0 mg/dL (interquartile range: 1.1-4.0). Patients with hepatitis C or nonalcoholic fatty liver disease had among the lowest ACLF incidence rates but had the highest short-term mortality. Conclusion: There is significant discordance in ACLF events by EASL and APASL criteria. The majority of patients with EASL-alone ACLF have preserved liver function, suggesting the need for more liver-specific ACLF criteria.
© 2019 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Author Disclosures
We confirm that none of the authors have any conflicts of interest or other relevant disclosures pertaining to this manuscript.
Figures
Comment in
-
Letter to the Editor: Defining Acute on Chronic Liver Failure: More Elusive Than Ever.Hepatology. 2019 Jul;70(1):450-451. doi: 10.1002/hep.30589. Hepatology. 2019. PMID: 30805952 No abstract available.
-
Letter to the Editor: Acute-on-Chronic Liver Failure: Conceptual Divergences.Hepatology. 2019 Sep;70(3):1076. doi: 10.1002/hep.30611. Hepatology. 2019. PMID: 30864173 No abstract available.
-
Letter to the Editor: Tale of Two ACLF Definitions: Choices Are Getting Clearer.Hepatology. 2019 Dec;70(6):2233-2235. doi: 10.1002/hep.30836. Hepatology. 2019. PMID: 31243776 No abstract available.
-
Letter to the Editor: Incidence and Mortality of Acute on Chronic Liver Failure Using Two Definitions in Patients With Compensated Cirrhosis.Hepatology. 2019 Dec;70(6):2235-2236. doi: 10.1002/hep.30837. Hepatology. 2019. PMID: 31243777 No abstract available.
-
Reply.Hepatology. 2019 Dec;70(6):2236-2238. doi: 10.1002/hep.30835. Hepatology. 2019. PMID: 31243784 Free PMC article. No abstract available.
References
-
- D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. Journal of hepatology 2006;44:217–231. - PubMed
-
- Lefton HB, Rosa A, Cohen M. Diagnosis and epidemiology of cirrhosis. Medical Clinics 2009;93:787–799. - PubMed
-
- Jalan R, Saliba F, Pavesi M, et al. Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure. Journal of hepatology 2014;61:1038–1047. - PubMed
-
- Moreau R, Jalan R, Gines P, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013;144:1426–1437.e9. - PubMed
-
- Sarin SK, Kedarisetty CK, Abbas Z, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver (APASL) 2014. Hepatology international 2014;8:453–471. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
