

The value of syntax score to predict new-onset atrial fibrillation in patients with acute coronary syndrome
- PMID: 30615236
- PMCID: PMC6931656
- DOI: 10.1111/anec.12622
The value of syntax score to predict new-onset atrial fibrillation in patients with acute coronary syndrome
Abstract
Background and aim: New-onset atrial fibrillation (NOAF) has been associated with poor outcome in patients with acute coronary syndromes (ACS). Also, Syntax score (SS) is a scoring system that is derived from angiographic images and is associated with long-term mortality and major adverse cardiac events. In this study, we aimed to assess the relationship between SS and NOAF with known predictors of atrial fibrillation.
Methods: In a prospective, single-center, cross-sectional study, 692 patients who were diagnosed with coronary artery disease for the first time were enrolled consecutively. NOAF was defined as atrial fibrillation, which was documented after hospital admission. SS was calculated by a computer software. Multivariable logistic regression analyzes were used to detect the relationship between variables and NOAF.
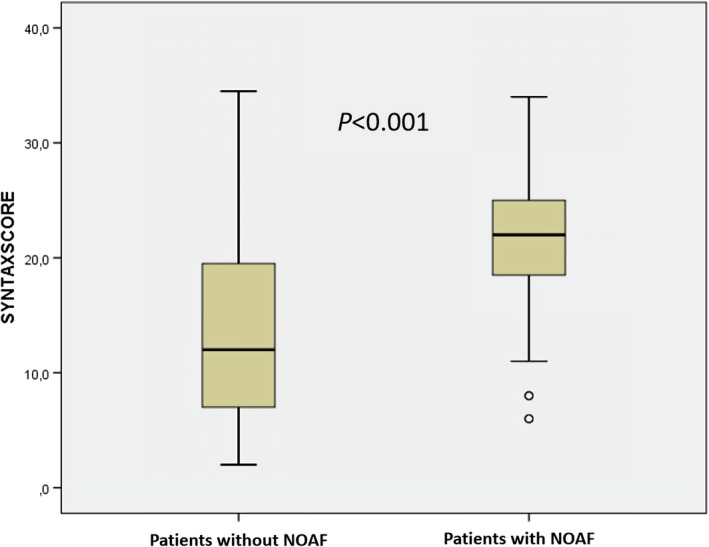
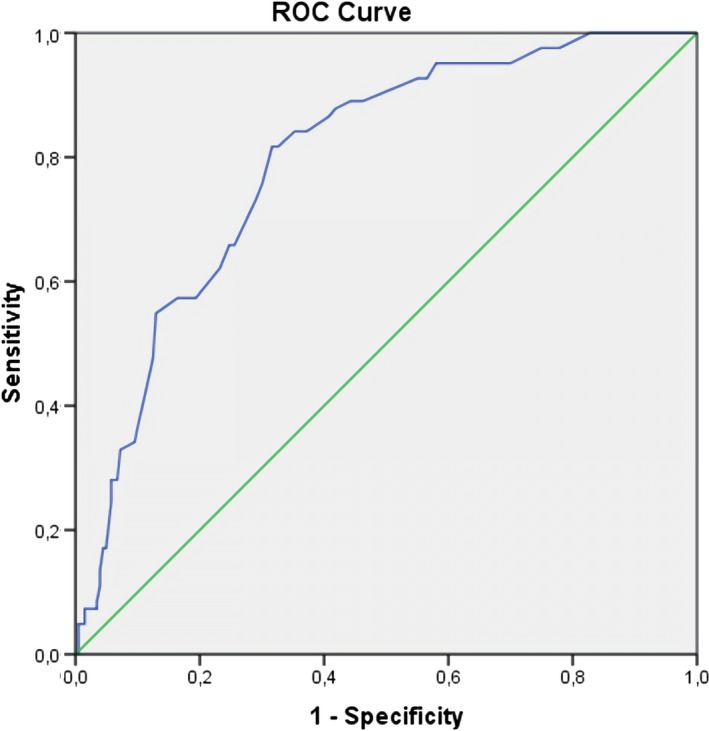
Results: New-onset atrial fibrillation was detected in 82 patients (11.8%). Patients with NOAF had higher SS (22, interquartile range 18.3-25.1, vs. 12, interquartile range 7-19.5, p < 0.001). According to multivariable logistic regression analysis for NOAF, SS were independently and significantly associated (OR, 1.103; 95% confidence interval, 1.047-1.163; p < 0.001). Other independent predictors of NOAF were TIMI flow <3, C reactive protein, left ventricular ejection fraction, left atrial volume index and E/E' ratio. The optimal cut-off value for SS was 18 for the development of NOAF with 82% sensitivity and 68% specificity (area under the curve: 0.795, 95% confidence interval 0.749-0.841, p < 0.001).
Conclusion: Syntax score may be helpful to identify for patients who would develop atrial fibrillation in the setting of ACS.
Keywords: SYNTAX Score; acute coronary syndrome; new-onset atrial fibrillation.
© 2019 Wiley Periodicals, Inc.
Conflict of interest statement
The Author(s) declare(s) that there is no conflict of interest.
Figures
References
-
- Alasady, M. , Abhayaratna, W. P. , Leong, D. P. , Lim, H. S. , Abed, H. S. , Brooks, A. G. , … Sanders, P. (2011). Coronary artery disease affecting the atrial branches is an independent determinant of atrial fibrillation after myocardial infarction. Heart Rhythm, 8(7), 955–960. 10.1016/j.hrthm.2011.02.016 - DOI - PubMed
-
- Amsterdam, E. A. , Wenger, N. K. , Brindis, R. G. , Casey, D. E. , Ganiats, T. G. , Holmes, D. R. , … Levine, G. N. (2014). 2014 AHA/ACC guideline for the management of patients with non–ST‐elevation acute coronary syndromes: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology, 64(24), e139–e228. - PubMed
-
- Aronson, D. , Boulos, M. , Suleiman, A. , Bidoosi, S. , Agmon, Y. , Kapeliovich, M. , … Suleiman, M. (2007). Relation of C‐reactive protein and new‐onset atrial fibrillation in patients with acute myocardial infarction. The American Journal of Cardiology, 100(5), 753–757. 10.1016/j.amjcard.2007.04.014 - DOI - PubMed
-
- Aronson, D. , Mutlak, D. , Bahouth, F. , Bishara, R. , Hammerman, H. , Lessick, J. , … Agmon, Y. (2011). Restrictive left ventricular filling pattern and risk of new‐onset atrial fibrillation after acute myocardial infarction. The American Journal of Cardiology, 107(12), 1738–1743. 10.1016/j.amjcard.2011.02.334 - DOI - PubMed
-
- Camm, A. J. , Kirchhof, P. , Lip, G. Y. H. , Schotten, U. , Savelieva, I. , Ernst, S. , … Zupan, I. (2010). Guidelines for the management of atrial fibrillation: The task force for the management of atrial fibrillation of the european society of cardiology (ESC). European Heart Journal, 31(19), 2369–2429. 10.1093/eurheartj/ehq278 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
