

Cardiometabolic Polygenic Risk Scores and Osteoarthritis Outcomes: A Mendelian Randomization Study Using Data From the Malmö Diet and Cancer Study and the UK Biobank
- PMID: 30615301
- PMCID: PMC6563114
- DOI: 10.1002/art.40812
Cardiometabolic Polygenic Risk Scores and Osteoarthritis Outcomes: A Mendelian Randomization Study Using Data From the Malmö Diet and Cancer Study and the UK Biobank
Abstract
Objective: To investigate the causal role of cardiometabolic risk factors in osteoarthritis (OA) using associated genetic variants.
Methods: We studied 27,691 adults from the Malmö Diet and Cancer Study (MDCS) and replicated novel findings among 376,435 adults from the UK Biobank. Trait-specific polygenic risk scores for low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol levels, triglyceride levels, body mass index (BMI), fasting plasma glucose (FPG) levels, and systolic blood pressure (BP) were used to test the associations of genetically predicted elevations in each trait with incident OA diagnosis (n = 3,559), OA joint replacement (n = 2,780), or both (total OA; n = 4,226) in Mendelian randomization (MR) analyses in the MDCS, and with self-reported and/or hospital-diagnosed OA (n = 65,213) in the UK Biobank. Multivariable MR, MR-Egger, and weighted median MR were used to adjust for potential pleiotropic biases.
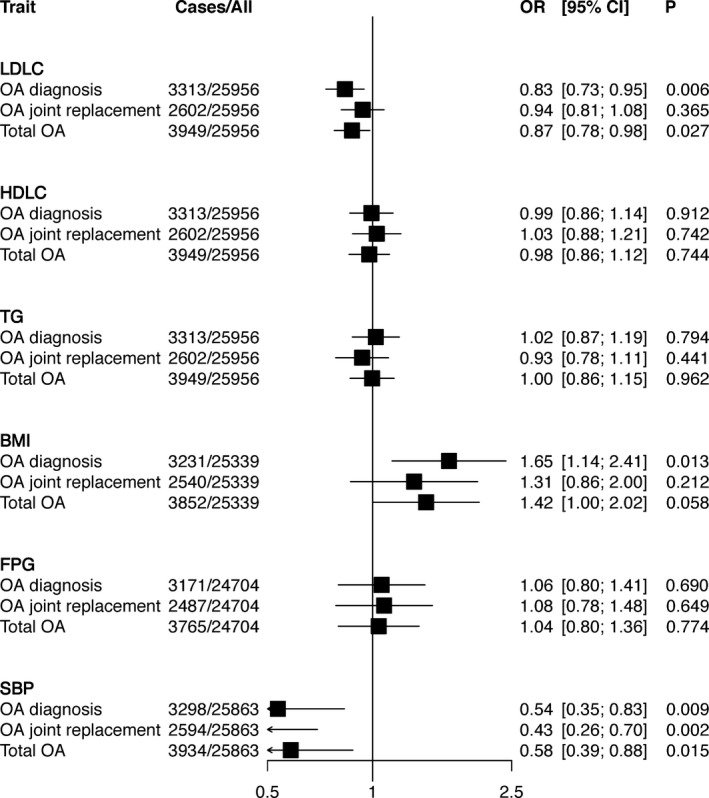
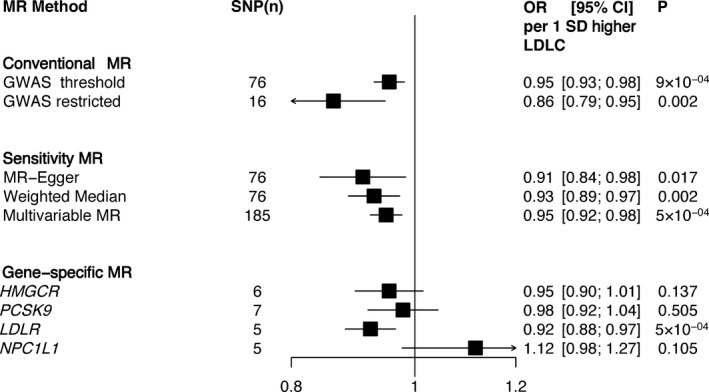
Results: In the MDCS, genetically predicted elevation in LDL cholesterol level was associated with a lower risk of OA diagnosis (odds ratio [OR] 0.83 [95% confidence interval (95% CI) 0.73-0.95] per 1SD increase) and total OA (OR 0.87 [95% CI 0.78-0.98]), which was supported by multivariable MR for OA diagnosis (OR 0.84 [95% CI 0.75-0.95]) and total OA (0.87 [95% CI 0.78-0.97]), and by conventional 2-sample MR for OA diagnosis (OR 0.86 [95% CI 0.75-0.98]). MR-Egger indicated no pleiotropic bias. Genetically predicted elevation in BMI was associated with an increased risk of OA diagnosis (OR 1.65 [95% CI 1.14-2.41]), while MR-Egger indicated pleiotropic bias and a larger association with OA diagnosis (OR 3.25 [1.26-8.39]), OA joint replacement (OR 3.81 [95% CI 1.39-10.4]), and total OA (OR 3.41 [95% CI 1.43-8.15]). No associations were observed between genetically predicted HDL cholesterol level, triglyceride level, FPG level, or systolic BP and OA outcomes. The associations with LDL cholesterol levels were replicated in the UK Biobank (OR 0.95 [95% CI 0.93-0.98]).
Conclusion: Our MR study provides evidence of a causal role of lower LDL cholesterol level and higher BMI in OA.
© 2019 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
References
-
- Zhuo Q, Yang W, Chen J, Wang Y. Metabolic syndrome meets osteoarthritis. Nat Rev Rheumatol 2012;8:729–37. - PubMed
-
- Kadam UT, Holmberg A, Blagojevic M, Nilsson PM, Akesson K. Risk factors for cardiovascular disease and future osteoarthritis‐related arthroplasty: a population‐based cohort study in men and women from Malmo, Sweden. Scand J Rheumatol 2011;40:478–85. - PubMed
-
- Aspden RM, Scheven BA, Hutchison JD. Osteoarthritis as a systemic disorder including stromal cell differentiation and lipid metabolism. Lancet 2001;357:1118–20. - PubMed
-
- Brandt KD, Doherty M, Lohmander S. Osteoarthritis. New York: Oxford University Press; 2003.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
