

Differences in tumor microenvironments between primary lung tumors and brain metastases in lung cancer patients: therapeutic implications for immune checkpoint inhibitors
- PMID: 30616523
- PMCID: PMC6322302
- DOI: 10.1186/s12885-018-5214-8
Differences in tumor microenvironments between primary lung tumors and brain metastases in lung cancer patients: therapeutic implications for immune checkpoint inhibitors
Abstract
Background: We aimed to compare intra- and extracranial responses to immune checkpoint inhibitors (ICIs) in lung cancer with brain metastases (BM), and to explore tumor microenvironments of the brain and lungs focusing on the programmed cell death-1 (PD-1)/programmed cell death ligand-1 (PD-L1) pathway.
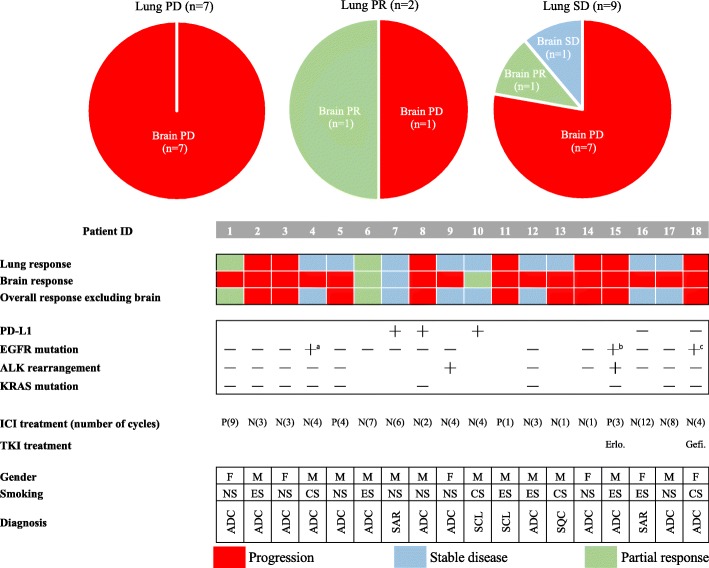
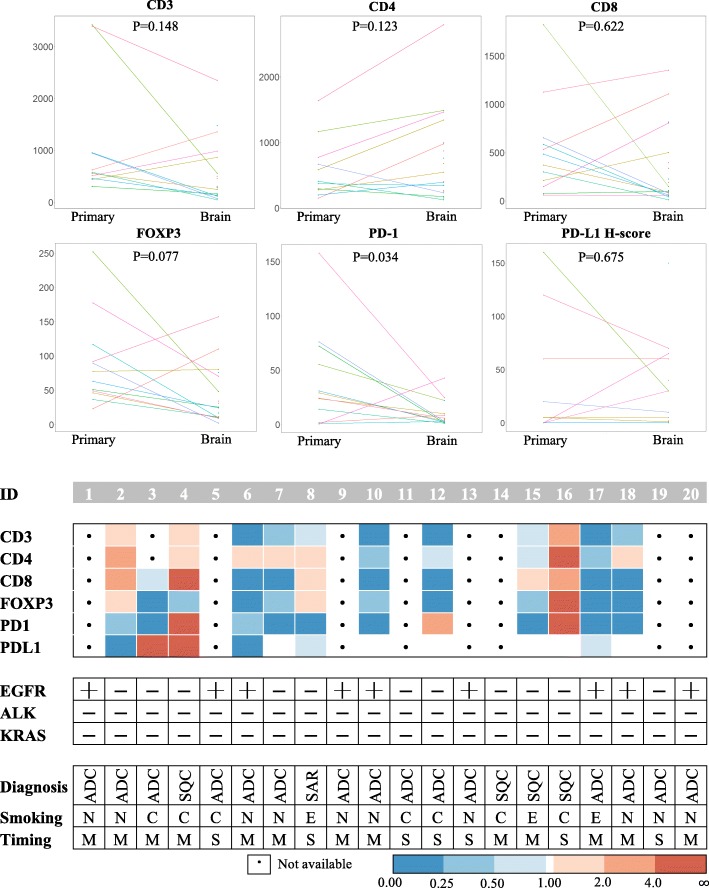
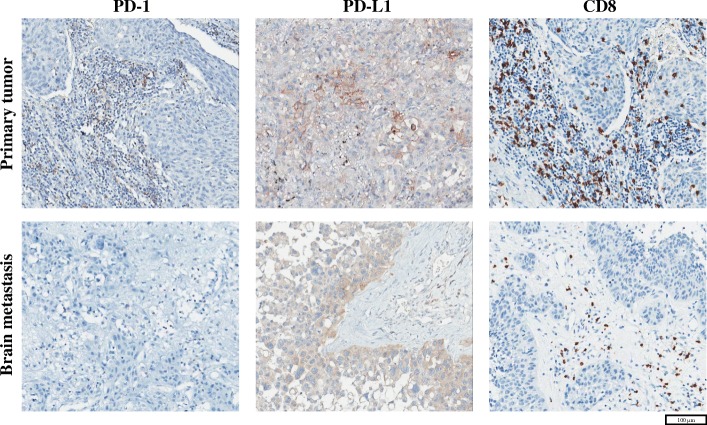
Methods: Two cohorts of lung cancer patients with BM were analyzed. Cohort 1 included 18 patients treated with nivolumab or pembrolizumab, and intra- and extracranial responses were assessed. Cohort 2 comprised 20 patients who underwent both primary lung surgery and brain metastasectomy. Specimens from cohort 2 were subjected to immunohistochemical analysis for the following markers: CD3, CD4, CD8, FOXP3, and PD-1 on tumor infiltrating lymphocytes (TIL) and PD-L1 on tumor cells.
Results: Seven patients (38.9%) in cohort 1 showed progressive disease in both primary and intracranial lesions. Although the other 11 patients exhibited a partial response or stable disease in the primary lesion, eight showed a progression in BM. Interestingly, PD-1+ TILs were significantly decreased in BM (P = 0.034). For fifteen patients with adenocarcinoma, more distinctive patterns were observed in CD3+ (P = 0.078), CD8+ (P = 0.055), FOXP3+ (P = 0.016), and PD-1+ (P = 0.016) TILs.
Conclusions: There may be discordant responses to an ICI of lung cancer between primary lung lesion and BM based on discrepancies in the tumor microenvironment. The diminished infiltration of PD-1+ TILs in tumor tissue within the brain may be one of the major factors that hinder the response to anti-PD-1 antibody in BM.
Keywords: Brain metastasis; Immunotherapy; Lung cancer; PD-1; PD-L1.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the SNUH Institutional Review Board (IRB approval number: H-1702-158-836) and was conducted in accordance with Declaration of Helsinki provisions. Written informed consent to participate in the study was obtained from each patient at admission.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Mathieu D, Kondziolka D, Cooper PB, Flickinger JC, Niranjan A, Agarwala S, Kirkwood J, Lunsford LD. Gamma knife radiosurgery for malignant melanoma brain metastases. Clin Neurosurg. 2007;54:241–247. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
