

Validation of the oncologic effect of hepatic resection for T2 gallbladder cancer: a retrospective study
- PMID: 30616645
- PMCID: PMC6323785
- DOI: 10.1186/s12957-018-1556-6
Validation of the oncologic effect of hepatic resection for T2 gallbladder cancer: a retrospective study
Abstract
Background: While extended cholecystectomy is recommended for T2 gallbladder cancer (GBC), the role of hepatic resection for T2 GBC is unclear. This study aimed to identify the necessity of hepatic resection in patients with T2 GBC.
Methods: Data of 81 patients with histopathologically proven T2 GBC who underwent surgical resection between January 1999 and December 2017 were enrolled from a retrospective database. Of these, 36 patients had peritoneal-side (T2a) tumors and 45 had hepatic-side (T2b) tumors. To identify the optimal surgical management method, T2 GBC patients were classified into the hepatic resection group (n = 44, T2a/T2b = 20/24) and non-hepatic resection group (n = 37, T2a/T2b = 16/21). The recurrence pattern and role of hepatic resection for T2 GBC were then investigated.
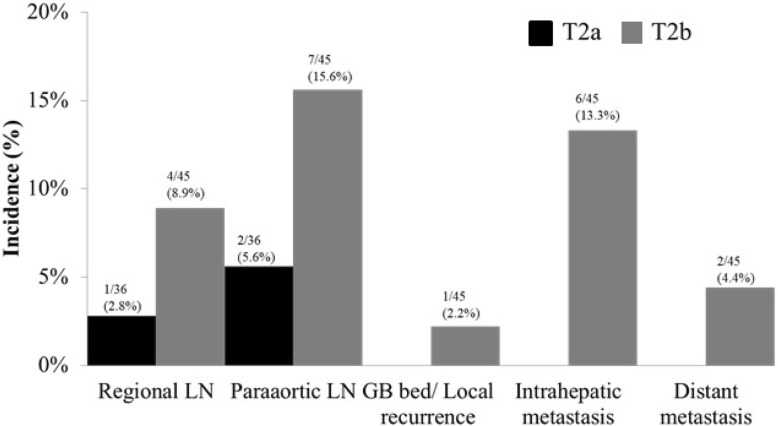
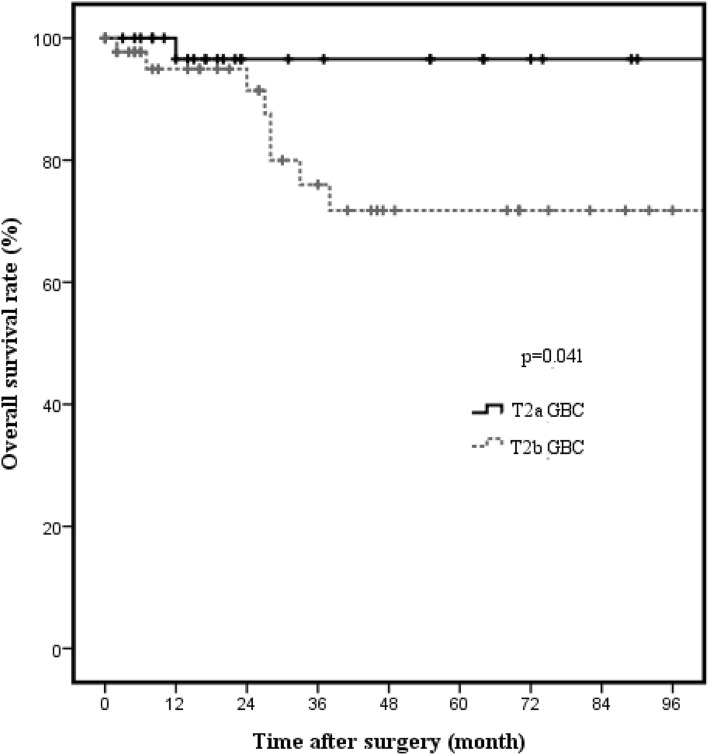
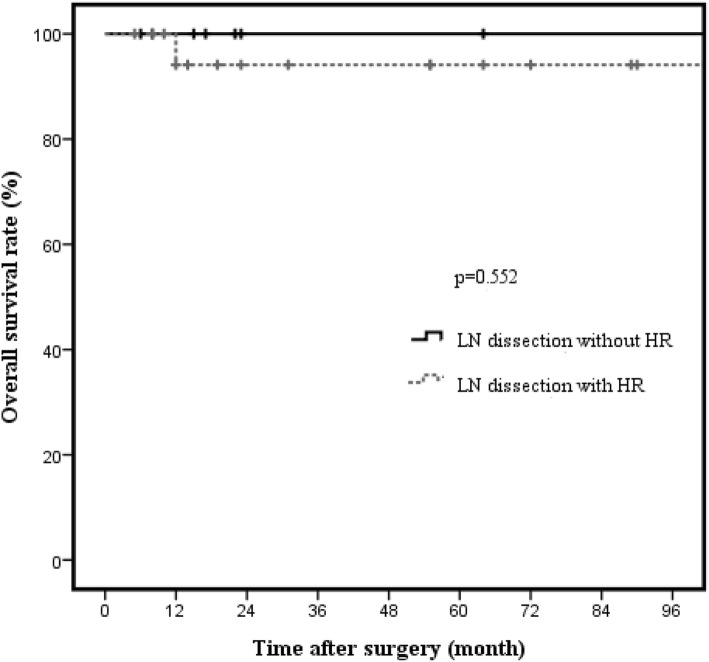
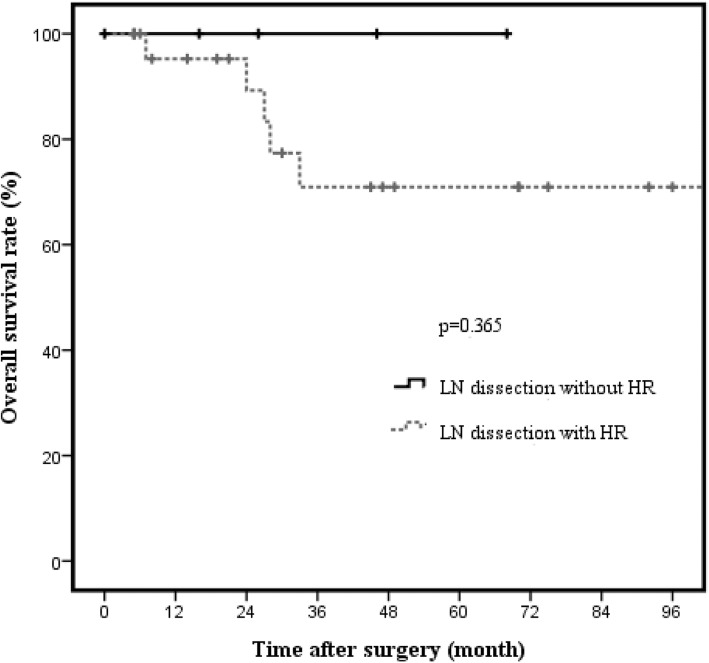
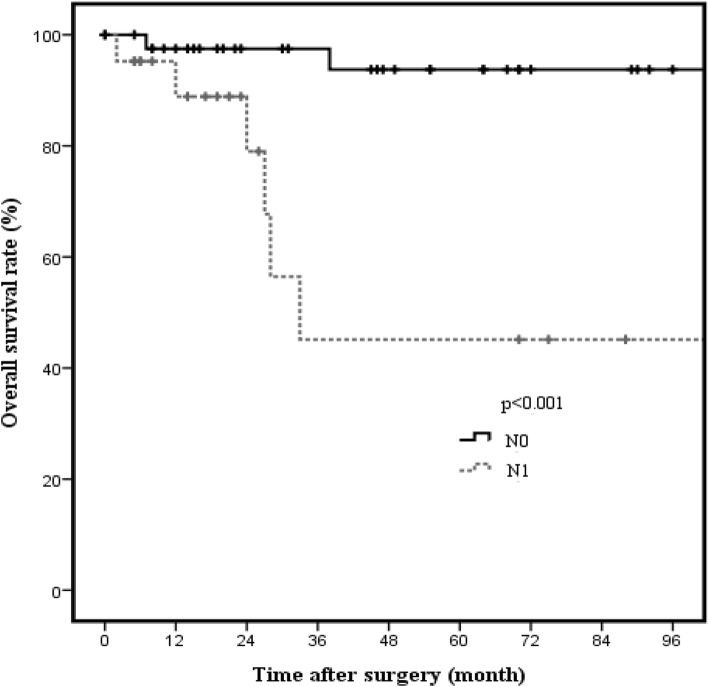
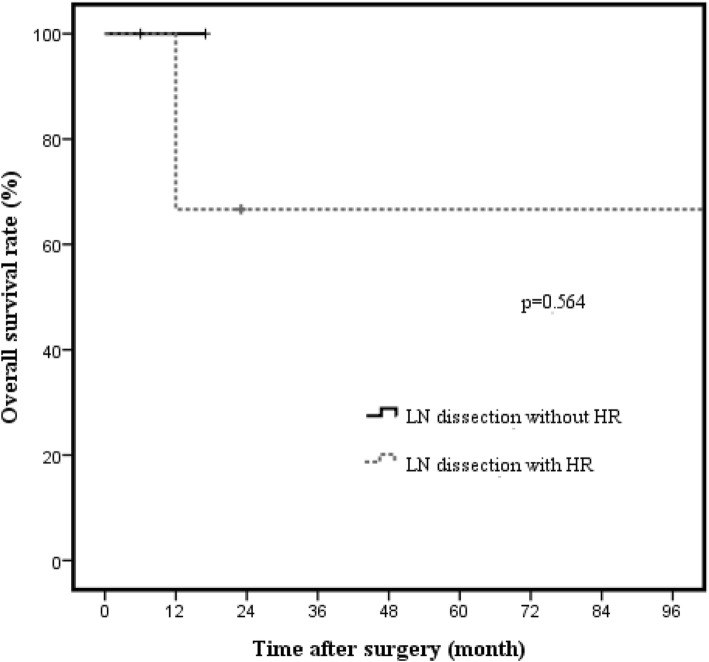
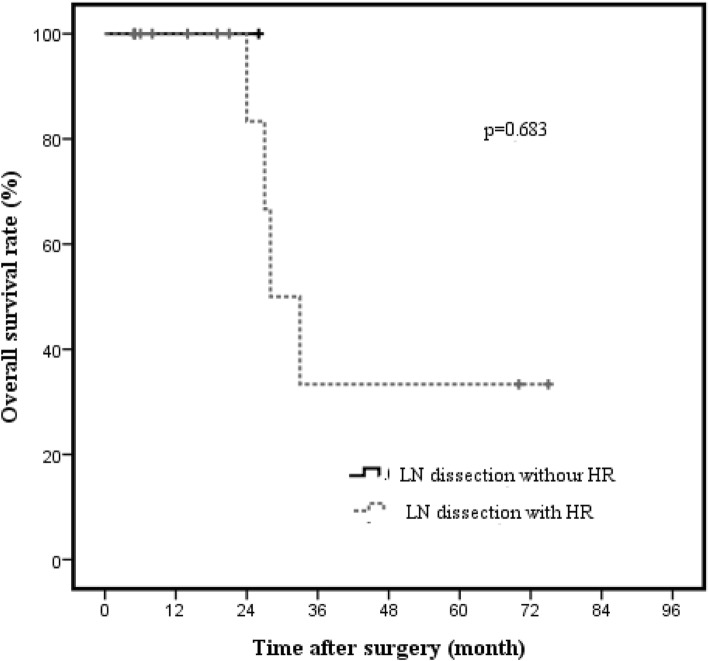
Results: Mean age of the patients was 69 (range 36-88) years, and the male-to-female ratio was 42:39 (male, 51.9%; female, 48.1%). Hepatic-side GBC had a higher rate of recurrence than peritoneal-side GBC (44.4% vs. 8.3%, p = 0.006). The most common type of recurrence in T2a GBC was para-aortic lymph node recurrence (n = 2, 5.6%); the most common types of recurrence in T2b GBC were para-aortic lymph node recurrence (n = 7, 15.6%) and intrahepatic metastasis (n = 6, 13.3%). Hepatic-side GBC patients had worse survival outcomes than peritoneal-side GBC patients (76.0% vs. 96.6%, p = 0.041). Hepatic resection had no significant treatment effect in T2 GBC patients (p = 0.272). Multivariate analysis showed that lymph node metastasis was the only significant prognostic factor (p = 0.002).
Conclusions: Hepatic resection is not essential for curative treatment in T2 GBC, and more systemic treatments are needed for GBC patients, particularly for those with T2b GBC.
Keywords: Gallbladder carcinoma; Hepatic resection; Surgical strategies.
Conflict of interest statement
Ethics approval and consent to participate
This retrospective study was approved by Institutional Review Board of the Gyeongsang National University Hospital (Approval no.: GNUH 2016-02-008). Patient informed consent was waived because of the retrospective nature of the study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Eckel F, Brunner T, Jelic S, Group EGW Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2011;22(Suppl 6):vi40–vi44. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
