

How are gender inequalities facing India's one million ASHAs being addressed? Policy origins and adaptations for the world's largest all-female community health worker programme
- PMID: 30616656
- PMCID: PMC6323796
- DOI: 10.1186/s12960-018-0338-0
How are gender inequalities facing India's one million ASHAs being addressed? Policy origins and adaptations for the world's largest all-female community health worker programme
Abstract
Background: India's accredited social health activist (ASHA) programme consists of almost one million female community health workers (CHWs). Launched in 2005, there is now an ASHA in almost every village and across many urban centres who support health system linkages and provide basic health education and care. This paper examines how the programme is seeking to address gender inequalities facing ASHAs, from the programme's policy origins to recent adaptations.
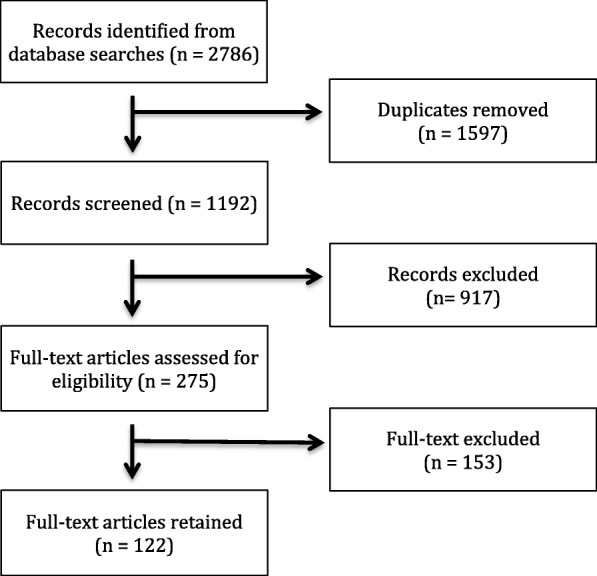
Methods: We reviewed all publically available government documents (n = 96) as well as published academic literature (n = 122) on the ASHA programme. We also drew from the embedded knowledge of this paper's government-affiliated co-authors, triangulated with key informant interviews (n = 12). Data were analysed thematically through a gender lens.
Results: Given that the initial impetus for the ASHA programme was to address reproductive and child health issues, policymakers viewed volunteer female health workers embedded in communities as best positioned to engage with beneficiaries. From these instrumentalist origins, where the programme was designed to meet health system demands, policy evolved to consider how the health system could better support ASHAs. Policy reforms included an increase in the number and regularity of incentivized tasks, social security measures, and government scholarships for higher education. Residential trainings were initiated to build empowering knowledge and facilitate ASHA solidarity. ASHAs were designated as secretaries of their village health committees, encouraging them to move beyond an all-female sphere and increasing their role in accountability initiatives. Measures to address gender based violence were also recently recommended. Despite these well-intended reforms and the positive gains realized, ongoing tensions and challenges related to their gendered social and employment status remain, requiring continued policy attention and adaptation.
Conclusions: Gender trade offs and complexities are inherent to sustaining CHW programmes at scale within challenging contexts of patriarchal norms, health system hierarchies, federal governance structures, and evolving aspirations, capacities, and demands from female CHWs. Although still grappling with significant gender inequalities, policy adaptations have increased ASHAs' access to income, knowledge, career progression, community leadership, and safety. Nonetheless, these transformative gains do not mark linear progress, but rather continued adaptations.
Keywords: Community health workers; Gender; Human resources for health; India; Policy analysis.
Conflict of interest statement
Ethics approval and consent to participate
Biomedical Science Research Ethics Committee of the University of the Western Cape, South Africa, approved the key informant interviews (reference number: BM17/6/18, rec number REC 130416-050). Our analysis of publically available government policy documents and published academic work are not human subject research. All participants provided informed consent.
Consent for publication
Not applicable
Competing interests
RV, GG, SS, and AS are employees of the National Health Systems Resource Centre, which is a technical support agency for the National Rural Health Mission, under the Government of India’s Ministry of Health and Family Welfare. The other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Schneider H, Okello D, Lehmann U. The global pendulum swing towards community health workers in low- and middle-income countries: a scoping review of trends, geographical distribution and programmatic orientations, 2005 to 2014. Hum Resour Health. 2016;14(1):65. doi: 10.1186/s12960-016-0163-2. - DOI - PMC - PubMed
-
- NHSRC. Update on ASHA programme, January. New Delhi; 2017. Available from: http://nhsrcindia.org/sites/default/files/Update%20on%20ASHA%20Programme.... Accessed 10 Apr 2017.
-
- George AS. Human resources for health: a gender analysis. Review Paper prepared for the Women and Gender Equity, and Health Systems, Knowledge Networks Networks (KNs) of the WHO Commission on the Social Determinants of Health. 2007. Available from: https://www.who.int/social_determinants/resources/human_resources_for_he....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
