

Hepatocellular Carcinoma Screening Is Associated With Increased Survival of Patients With Cirrhosis
- PMID: 30616961
- PMCID: PMC6431264
- DOI: 10.1016/j.cgh.2018.10.031
Hepatocellular Carcinoma Screening Is Associated With Increased Survival of Patients With Cirrhosis
Abstract
Background & aims: Hepatocellular carcinoma (HCC) screening of patients with cirrhosis is recommended by professional societies to increase detection of early stage tumors and survival, but is underused in clinical practice.
Methods: We conducted a retrospective cohort study of 13,714 patients diagnosed with HCC from 2003 through 2013 included in the Surveillance, Epidemiology, and End Results Program-Medicare database. We characterized receipt of HCC screening in the 3 years before HCC diagnosis using mutually exclusive categories (consistent vs inconsistent vs no screening) and the proportion of time covered with screening. Correlates for screening receipt were assessed using a multivariable 2-part regression model. We examined the association between screening receipt and early detection of tumors using multivariable logistic regression. We evaluated associations between screening receipt and overall survival using a Cox proportional hazards model, after adjustments for effects of lead-time bias and length-time bias on survival rate estimators.
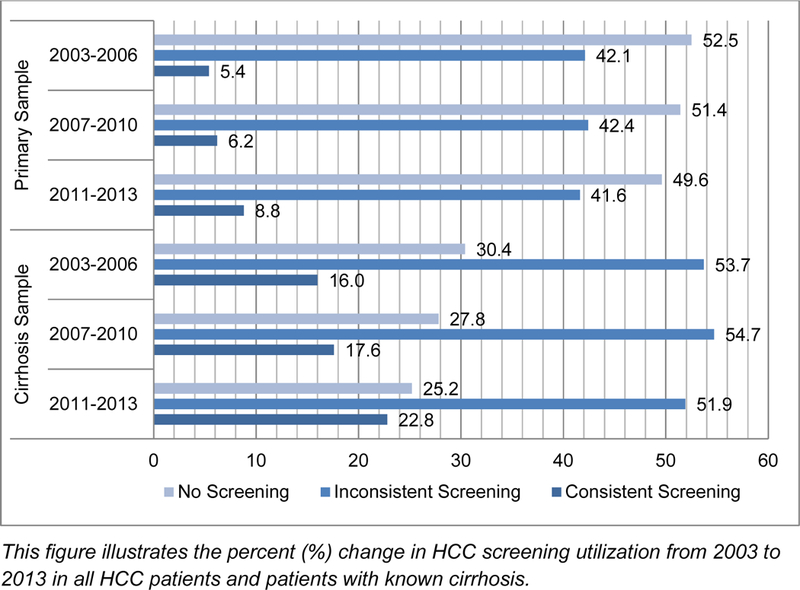
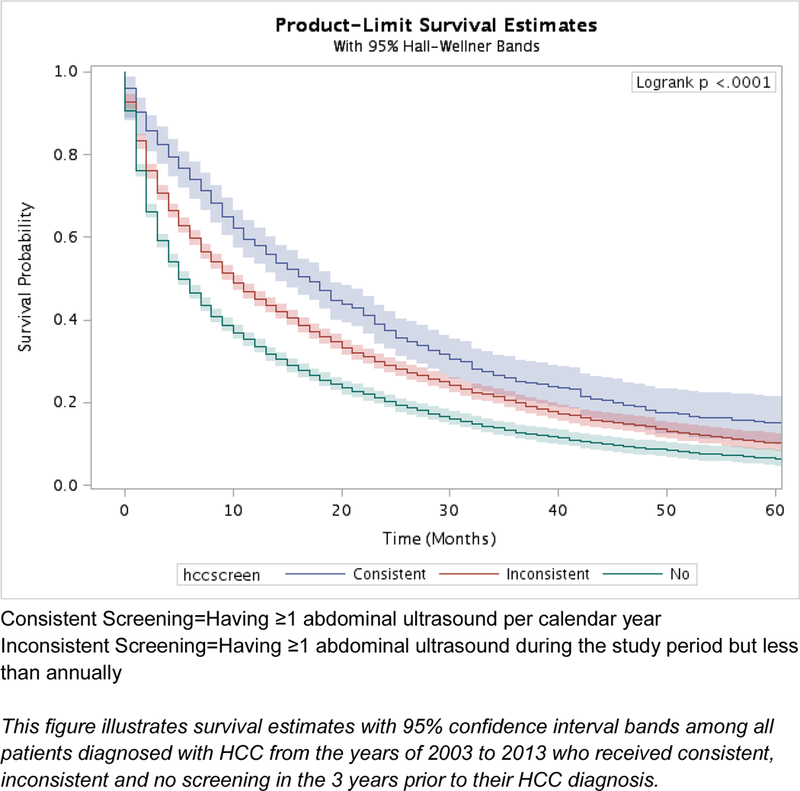
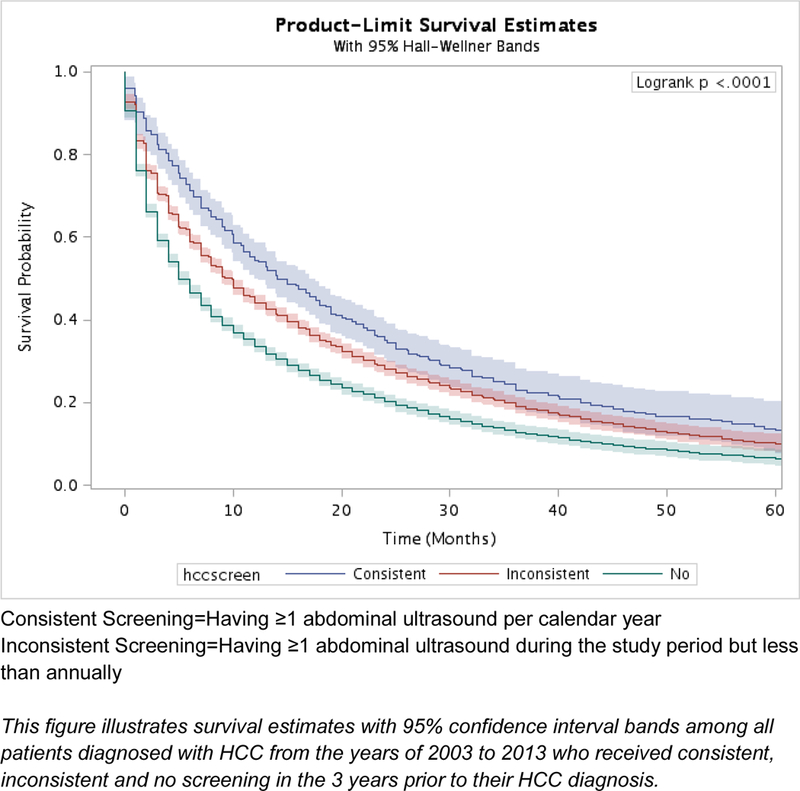
Results: Most patients with cirrhosis (51.1%) did not receive any screening in the 3 years before a diagnosis of HCC, and only 6.8% of patients underwent consistent annual screening. The proportion with consistent screening increased from 5.4% in 2003 to 2006 to 8.8% in 2011 to 2013 (P < .001). The mean proportion of time covered was 13.4% overall, which increased from 11.7% in 2003 to 2006 to 15.2% in 2011 to 2013. Receipt of consistent screening was associated with detection of early stage tumors (odds ratio, 1.98; 95% CI, 1.68-2.33) and a reduced risk of death after correction for lead-time bias (hazard ratio, 0.76; 95% CI, 0.70-0.83). Inconsistent screening was associated with a slightly smaller increase in early detection of HCC (odds ratio, 1.31; 95% CI, 1.20-1.43) and a reduced risk of death (hazard ratio, 0.86; 95% CI, 0.83-0.90). After correction for lead- and length-time biases, higher proportions of patients with consistent (23%; 95% CI, 21%-25%) and inconsistent screening (19%; 95% CI, 19%-20%) survived for 3 years compared with patients without screening (13%; 95% CI, 12%-14%).
Conclusions: In an analysis of the Surveillance, Epidemiology, and End Results Program-Medicare database, we found HCC screening to be underused for patients with cirrhosis. This contributes to detection of liver tumors at later stages and shorter times of survival. However, the proportion of patients screened for HCC has increased over time.
Keywords: Liver Cancer; SEER Database Analysis; Screening; Ultrasound.
Copyright © 2019 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- El-Serag HB, Davila JA, Petersen NJ, McGlynn KA. The continuing increase in the incidence of hepatocellular carcinoma in the United States: an update. Ann Intern Med 2003;139(10):817–823. doi:139/10/817 [pii] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
