

Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis
- PMID: 30617123
- PMCID: PMC6322065
- DOI: 10.1136/bmj.k5120
Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis
Abstract
Objectives: To compare re-rupture rate, complication rate, and functional outcome after operative versus nonoperative treatment of Achilles tendon ruptures; to compare re-rupture rate after early and late full weight bearing; to evaluate re-rupture rate after functional rehabilitation with early range of motion; and to compare effect estimates from randomised controlled trials and observational studies.
Design: Systematic review and meta-analysis.
Data sources: PubMed/Medline, Embase, CENTRAL, and CINAHL databases were last searched on 25 April 2018 for studies comparing operative versus nonoperative treatment of Achilles tendon ruptures.
Study selection criteria: Randomised controlled trials and observational studies reporting on comparison of operative versus nonoperative treatment of acute Achilles tendon ruptures.
Data extraction: Data extraction was performed independently in pairs, by four reviewers, with the use of a predefined data extraction file. Outcomes were pooled using random effects models and presented as risk difference, risk ratio, or mean difference, with 95% confidence interval.
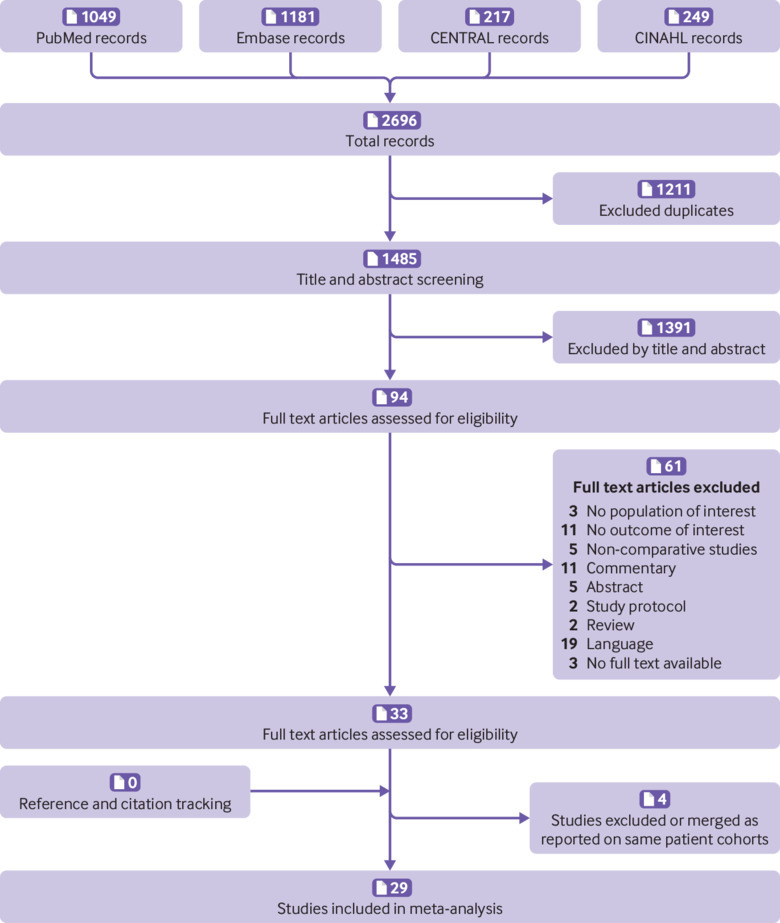
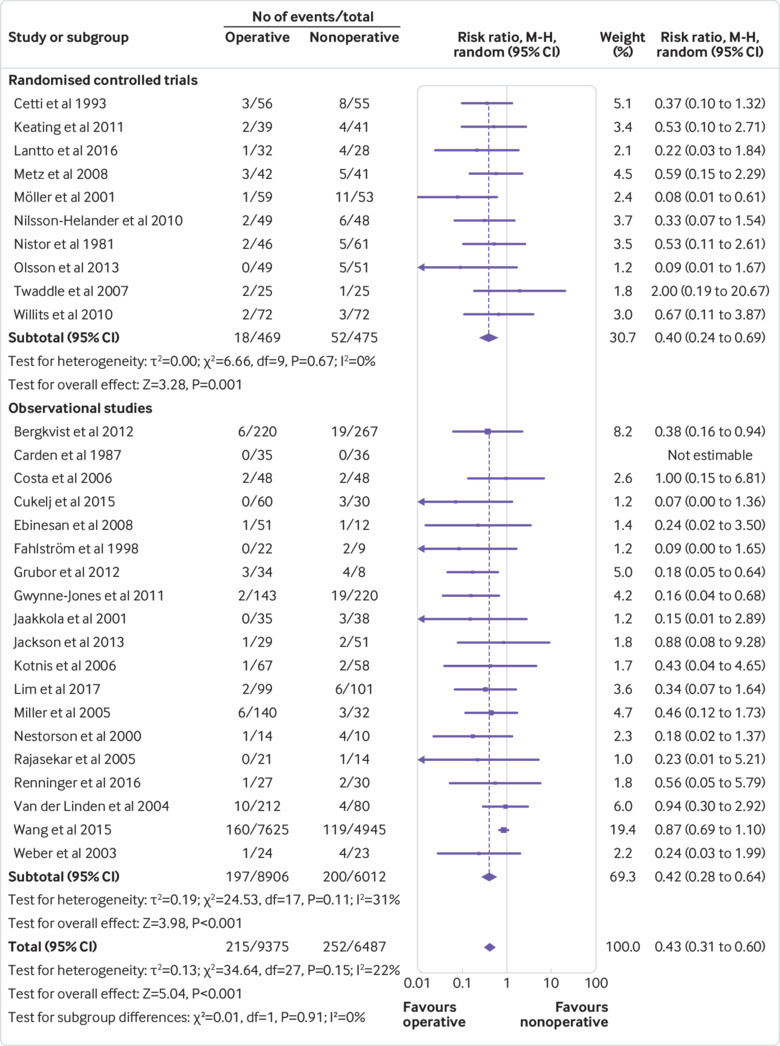
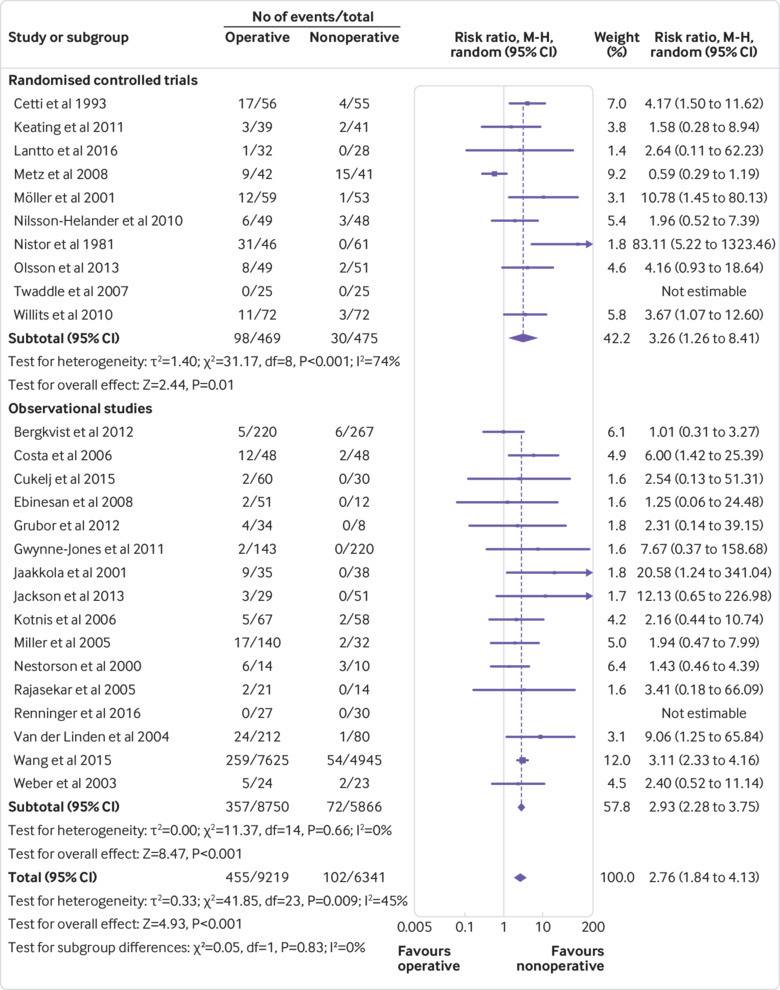
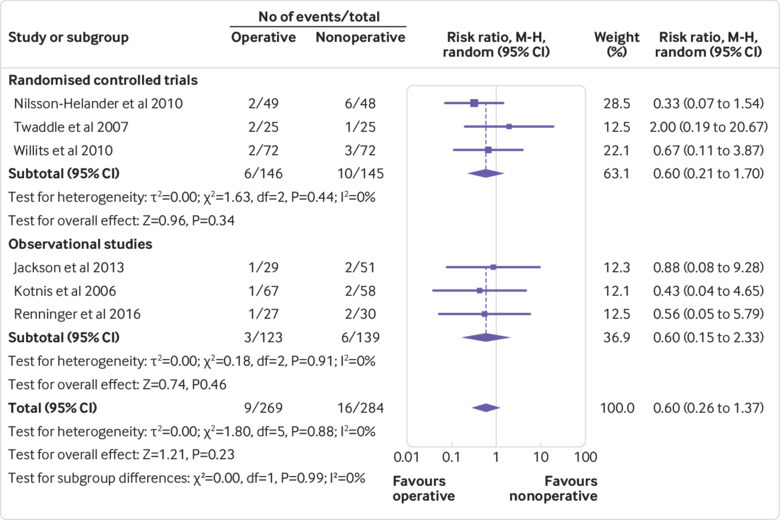
Results: 29 studies were included-10 randomised controlled trials and 19 observational studies. The 10 trials included 944 (6%) patients, and the 19 observational studies included 14 918 (94%) patients. A significant reduction in re-ruptures was seen after operative treatment (2.3%) compared with nonoperative treatment (3.9%) (risk difference 1.6%; risk ratio 0.43, 95% confidence interval 0.31 to 0.60; P<0.001; I2=22%). Operative treatment resulted in a significantly higher complication rate than nonoperative treatment (4.9% v 1.6%; risk difference 3.3%; risk ratio 2.76, 1.84 to 4.13; P<0.001; I2=45%). The main difference in complication rate was attributable to the incidence of infection (2.8%) in the operative group. A similar reduction in re-rupture rate in favour of operative treatment was seen after both early and late full weight bearing. No significant difference in re-rupture rate was seen between operative and nonoperative treatment in studies that used accelerated functional rehabilitation with early range of motion (risk ratio 0.60, 0.26 to 1.37; P=0.23; I2=0%). No difference in effect estimates was seen between randomised controlled trials and observational studies.
Conclusions: This meta-analysis shows that operative treatment of Achilles tendon ruptures reduces the risk of re-rupture compared with nonoperative treatment. However, re-rupture rates are low and differences between treatment groups are small (risk difference 1.6%). Operative treatment results in a higher risk of other complications (risk difference 3.3%). The final decision on the management of acute Achilles tendon ruptures should be based on patient specific factors and shared decision making. This review emphasises the potential benefits of adding high quality observational studies in meta-analyses for the evaluation of objective outcome measures after surgical treatment.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Surgery or conservative management for Achilles tendon rupture?BMJ. 2019 Jan 7;364:k5344. doi: 10.1136/bmj.k5344. BMJ. 2019. PMID: 30617220 No abstract available.
References
-
- Ganestam A, Kallemose T, Troelsen A, Barfod KW. Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013. A nationwide registry study of 33,160 patients. Knee Surg Sports Traumatol Arthrosc 2016;24:3730-7. 10.1007/s00167-015-3544-5 - DOI - PubMed
-
- Khan RJ, Carey Smith RL. Surgical interventions for treating acute Achilles tendon ruptures. Cochrane Database Syst Rev 2010;(9):CD003674. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous