

Moving From Heart Failure Guidelines to Clinical Practice: Gaps Contributing to Readmissions in Patients With Multiple Comorbidities and Older Age
- PMID: 30618487
- PMCID: PMC6299336
- DOI: 10.1177/1179546818809358
Moving From Heart Failure Guidelines to Clinical Practice: Gaps Contributing to Readmissions in Patients With Multiple Comorbidities and Older Age
Abstract
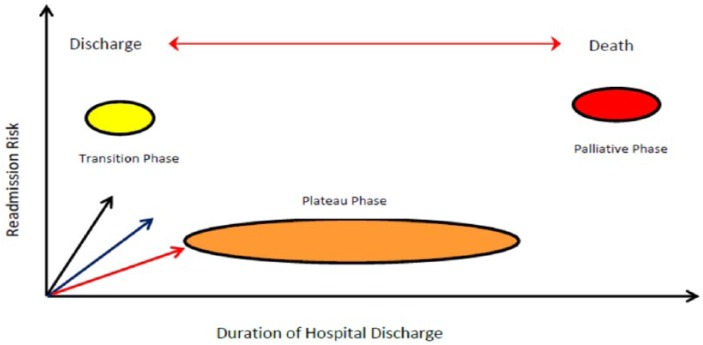
This feature article for the thematic series on congestive heart failure (CHF) readmissions aims to outline important gaps in guidelines for patients with multiple comorbidities and the elderly. Congestive heart failure diagnosis manifests as a 3-phase journey between the hospital and community, during acute, chronic stable, and end-of-life (palliative) phases. This journey requires in variable intensities a combination of multidisciplinary care within tertiary hospital or ambulatory care from hospital outpatients or primary health services, within the general community. Management goals are uniform, ie, to achieve the lowest New York Heart Association class possible, with improvement in ejection fraction, by delivering gold standard therapies within a CHF program. Comorbidities are an important common denominator that influences outcomes. Comorbidities include diabetes mellitus, chronic obstructive airways disease, chronic renal impairment, hypertension, obesity, sleep apnea, and advancing age. Geriatric care includes the latter as well as syndromes such as frailty, falls, incontinence, and confusion. Many systems still fail to comprehensively achieve all aspects of such programs. This review explores these factors.
Keywords: comorbidity; elderly; geriatric; readmissions; translating guidelines; translational research.
Conflict of interest statement
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
Appendix 1
Additional references for Table 1
-
- McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham study. N Engl J Med. 1971;285:1441–1446. - PubMed
-
- Ho K, Anderson KM, Kannel WB, Grossman W, Levy D. Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation. 1993;88:107–115. - PubMed
-
- Ho KKL, Pinsky JL, Kannel WB, Levy D. The epidemiology of heart failure: the Framingham Study. J Am Coll Cardiol. 1993;22:A6–A13. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, et al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–1402. - PubMed
References
-
- Desai AS, Stevenson LW. Rehospitalization for heart failure: predict or prevent? Circulation. 2012;126:501–506. - PubMed
-
- Cintron G, Johnson G, Francis G, Cobb F, Cohn JN. Prognostic significance of serial changes in left ventricular ejection fraction in patients with congestive heart failure. The V-HeFT VA Cooperative Studies Group. Circulation. 1993;87:VI17–VI23. - PubMed
-
- Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics—2008 update: a report from the American Heart Association statistics committee and stroke statistics subcommittee. Circulation. 2008;117:e25–e146. - PubMed
-
- Chaudhry SP, Stewart GC. Advanced heart failure: prevalence, natural history, and prognosis. Heart Fail Clin. 2016;12:323–333. - PubMed
LinkOut - more resources
Full Text Sources
Medical
